Back Clinic Migraine Team. This is a genetic neurological disease characterized by episodes called Migraine attacks. They are quite different from regular headaches, which are non-migrainous. About 100 million people suffer from headaches in the U.S., And 37 million of these people suffer migraines. The World Health Organization estimates that 18 percent of women and 7 percent of men in the U.S. suffer.
They are called primary headaches because the pain is not caused by a disorder or disease, i.e., a brain tumor or head injury. Some cause pain only on the right side or left side of the head. In contrast, others result in pain everywhere. Individuals that suffer can have moderate or severe pain but usually can’t participate in regular activities because of the pain.
When a migraine strikes, a quiet, dark room may help with the symptoms. Migraines can last for four hours or can last for days. The range of time someone is affected by an attack is actually longer than the migraine itself. This is because a pre-monitory or build-up and a post-drome can last for one to two days.
Origin: The most common cause of�migraines/headaches�can relate to neck complications. From spending excessive time looking down at a laptop, desktop, iPad, and even from constant texting, an incorrect posture for extended periods of time can begin to place pressure on the neck and upper back leading to problems that can cause headaches. The majority of these type of headaches occurs as a result of tightness between the shoulder blades, which in turn causes the muscles on the top of the shoulders to also tighten and radiate pain into the head.
Arteriovenous malformations and expanding aneurysms
Lupus cerebritis
Venous sinus thrombosis
Cervical fracture or malformation
Fracture or dislocation
Occipital neuralgia
Vertebral artery dissection
Chiari malformation
Metabolic
Hypoglycemia
Hypercapnea
Carbon monoxide
Anoxia
Anemia
Vitamin A toxicity
Glaucoma
Subarachnoid Hemorrhage
Usually due to ruptured aneurysm
Sudden onset of severe pain
Often vomiting
Patient appears ill
Often nuchal rigidity
Refer for CT and possibly lumbar puncture
Meningitis
Patient appears ill
Fever
Nuchal rigidity (except in elderly and young children)
Refer for lumbar puncture – diagnostic
Neoplasms
Unlikely cause of HA in average patient population
Mild and nonspecific head pain
Worse in the morning
May be elicited by vigorous head shaking
If focal symptoms, seizures, focal neurologic signs, or evidence of increased intracranial pressure are present rule our neoplasm
Subdural Or Epidural Hemorrhage
Due to hypertension, trauma or defects in coagulation
Most often occurs in the context of acute head trauma
Onset of symptoms may be weeks or months after an injury
Differentiate from the common post-concussion headache
Post-Concussive HA may persist for weeks or months after an injury and be accompanied by dizziness or vertigo and mild mental changes, which will all subside
Exquisite tenderness and/or swelling over the temporal or occipital arteries
Evidence of arterial insufficiency in the distribution of branches of the cranial vessels
High ESR
Cervical Region HA
Neck trauma or with symptoms or signs of cervical root or cord compression
Order MR or CT cord compression due to fracture or dislocation
Cervical instability
Order cervical spine x-rays lateral flexion and extension views
Ruling Out Dangerous HA
Rule our history of serious head or neck injury, seizures or focal neurologic symptoms, and infections that may predispose to meningitis or brain abscess
Check for fever
Measure blood pressure (concern if diastolic >120)
Ophthalmoscopic exam
Check neck for rigidity
Auscultate for cranial bruits.
Complete neurologic examination
If needed order complete blood cell count, ESR, cranial or cervical imaging
Episodic Or Chronic?
<15 days per month = Episodic
>15 days per month = Chronic
Migraine HA
Generally due to dilation or distension of cerebral vasculature
Serotonin In Migraine
AKA 5-hydroxytryptamine (5-HT)
Serotonin becomes depleted in migraine episodes
IV 5-HT can stop or reduce severity
Migraine With Aura
History of at least 2 attacks fulfilling the following criteria
One of the following fully reversible aura symptoms:
Visual
Somatic sensory
Speech or language difficulty
Motor
Brain stem
2 of the following 4 characteristics:
1 aura symptom spreads gradually over ?5 min, and/or 2 symptoms occur in succession
Each individual aura symptom lasts 5-60 min
1 aura symptom is unilateral
Aura accompanied or followed in <60 min by headache
Not better accounted for by another ICHD-3 diagnosis, and TIA excluded
Migraine Without Aura
History of at least 5 attacks fulfilling the following criteria:
Headache attacks lasting 4-72 h (untreated or unsuccessfully treated)
Unilateral pain
Pulsing/pounding quality
Moderate to severe pain intensity
Aggravation by or causing avoidance of routine physical activity
During headache nausea and/or sensitivity to light and sound
Not better accounted for by another ICHD-3 diagnosis
Cluster Headache
Severe unilateral orbital, supraorbital and/or temporal pain
�Like an ice pick stabbing me the eye�
Pain lasts 15-180 minutes
At least one of the following on the side of headache:
Conjunctival injection
Facial sweating
Lacrimation
Miosis
Nasal congestion
Ptosis
Rhinorrhea
Eyelid edema
History of similar headaches in the past
Tension Headache
Headache pain accompanied by two of the following:
Pressing/tightening (non-pulsing) quality
�Feels like a band around my head�
Bilateral location
Not aggravated by routine physical activity
Headache should be lacking:
Nausea or vomiting
Photophobia and phonophobia (one or the other may be present)
History of similar headaches in the past
Rebound Headache
Headache occurring on ?15 days a month in a patient with a pre-existing headache disorder
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache
Due to medication overuse/withdrawal
Not better accounted for by another ICHD-3 diagnosis
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
Headaches are very common health issues, and lots of people treat themselves by using basic painkillers, drinking additional water, with rest, or by simply waiting for the headache to go away on its own. As a matter of fact, a headache is among the most common reasons for doctor office visits.
Just about everyone will experience a headache sometime during their life. Most headaches are not caused by serious or sinister conditions. However, people understandably worry if headaches feel different, whether they’re especially severe, particularly frequent or unusual in any other manner. But, the most common concern is whether the headache may be a symptom of an underlying health issue, such as a brain tumor.
The following article discusses headaches generally. It explains the various types of headaches you may experience and describes those very rare situations where a headache may be a symptom of a serious disease.
Types of Headaches
Headaches can be categorized as primary, or they can be classified as secondary, meaning they are a side-effect of another injury or condition.
A healthcare professional can usually determine the possible cause of your headaches from speaking to you and examining you. When they have found the cause then you’ll have the ability to decide the best treatment approach for your head pain symptoms. This may involve taking drugs only when you get the headaches, taking daily medication to stop them altogether, and/or even stopping medication you’re already taking. Very occasionally, headaches may need further diagnosis to rule out more serious underlying causes. Chiropractic care and physical therapy are also commonly utilized to help treat headaches. Below, we will discuss the different types of headaches.
Primary Headaches
The most common types of headaches, by far, are tension headaches and migraines.
Tension Headaches
Tension headaches are generally felt as a band around the forehead. They may last for many days. They may be tiring and uncomfortable, but they don’t normally disturb sleep. Most people can carry on working with a tension headache. These often have a tendency to worsen as the day progresses, however, they aren’t usually made worse with physical activities, though it’s not strange to be somewhat sensitive to bright light or noise.
Migraines
Migraines are also very common types of headaches. A typical migraine is described as a throbbing sensation. Headaches which are one-sided, headaches which throb and headaches that make you feel sick are more inclined to be migraines compared to anything else. Migraines are often severe enough to be disabling. Some individuals will need to go to bed to sleep off their aggravation.
Cluster Headaches
Cluster headaches are extremely severe headaches, sometimes called “suicide headaches”. They occur in clusters, often every day for a number of days or maybe weeks. Then they vanish for weeks on end. These types of headaches are rare and often occur particularly in adult male smokers. They’re intense, one-sided headaches, which are very disabling, meaning they stop routine activity. People often describe them as the worst pain they have ever felt. Cluster headaches are typically one-sided. Patients frequently have a red watery eye on the other hand, a stuffy runny nose and a droopy eyelid.
Chronic Tension Headaches
Chronic tension headaches (or chronic daily headache) is generally caused by muscle tension in the back of the neck and affects women more frequently than men. Chronic means that the problem is persistent and ongoing. These headaches can develop due to neck injuries or tiredness and may worsen with drug/medication overuse. A headache that occurs virtually every day for 3 weeks or more is known as a chronic daily headache or a chronic tension headaches.
Medication-Overuse Headaches
Medication-overuse headaches or medication-induced aggravation, is an unpleasant and long-term headache. It’s brought on by taking painkillers usually meant for headaches. Unfortunately, when painkillers are taken regularly for headaches, the body reacts by creating additional pain sensors in the brain. Finally, the pain sensors are so many that the head becomes super-sensitive and the headache won’t go away. Individuals who have these headaches often take an increasing number of painkillers to attempt and feel much better. But, the painkillers may have regularly long ceased to work. Medication-overuse headaches are the most common cause of secondary headache.
Exertional Headaches/Sexual Headaches
Exertional headaches are headaches associated with physical activity. They may get severe very quickly following a strenuous activity like coughing, running, with intercourse, and straining with bowel movements. They’re more commonly experienced by patients that also have migraines, or who have relatives with migraine.
Headaches associated with sex particularly worry patients. They can occur as sex starts, at orgasm, or following sex. Headaches at orgasm would be the most common type. They are generally acute, at the back of the head, behind the eyes or all around. They last about twenty minutes and aren’t usually an indication of any other underlying health issues or problems.
Exertional and sexual intercourse-related headaches aren’t typically an indication of serious underlying problems. Very occasionally, they can be a sign that there is a leaky blood vessel on the surface of the brain. As a result, if they are marked and repeated, it’s sensible to talk about them with your healthcare professional.
Primary Stabbing Headaches
Primary traumatic headaches are sometimes called “ice-pick headaches” or “idiopathic stabbing headache”. The term “idiopathic” is used by doctors for something that comes without a clear cause. These are brief, stabbing headaches that are extremely sudden and severe. They generally last between 5 and 30 seconds and they occur at any time of the day or night. They feel as though a sharp object, like an ice pick, is being stuck into your head. They frequently occur in or just behind the ear and they are sometimes quite frightening. Even though they aren’t migraines they’re more prevalent in those who suffer from migraines, nearly half of individuals who experience migraines have principal stabbing headaches.
They are often felt at the place on the head where the migraines have a tendency to happen. Primary stabbing headaches are too brief to take care of, even though migraine prevention medications may reduce their number.
Hemicrania Continua
Hemicrania continua is a major chronic daily headache. It typically induces a continuous but shifting pain on one side of the brain. The pain is generally continuous with episodes of severe pain, which can last between 20 minutes and several days. During those episodes of severe pain there may be other symptoms, such as watering or redness of the eye, runny or blocked nose, and drooping of the eyelid, around precisely the same side as the aggravation. Similar to a migraine, there may also be sensitivity to light, feeling sick, such as nausea, and being sick, such as vomiting. The headaches do not go away but there may be periods when you don’t have any headaches. Hemicrania continua headaches respond to medicine called indometacin.
Trigeminal Neuralgia
Trigeminal neuralgia causes facial pain. The pain consists of very short bursts of electric shock-like sensations in the face, particularly at the area of the eyes, nose, scalp, brow, lips or limbs. It’s usually one-sided and is more common in people over age 50. It may be triggered by touch or a light breeze on the surface area.
Headache Causes
Occasionally, headaches have underlying causes, and treatment of the headache involves treating the cause. Individuals often fear that headaches are caused by serious illness, or by high blood pressure. Both of these are extremely uncommon causes of headache, really increased blood pressure usually causes no symptoms in any way.
Chemicals, Drugs and Substance Withdrawal
Headaches can be because of a substance, or its withdrawal, for example:
Carbon monoxide, that is made by gas heaters which aren’t properly ventilated
Drinking alcohol, with headache often experienced the morning afterwards
Deficiency of body fluid or dehydration
Headaches Due to Referred Pain
Some headaches may be caused by pain in some other portion of the head, such as ear or tooth pain, pain in the jaw joint and pain in the neck.
Sinusitis is also a frequent cause of headaches. The sinuses are “holes” in the skull which are there to stop it from becoming too heavy for the neck to transport around. They are lined with mucous membranes, such as the lining of the nose, and this creates mucus in response to colds or allergy. The liner membranes also swell and can block the drainage of the mucus out of the space. It subsequently becomes cracked and infected, resulting in headache. The headache of sinusitis is often felt at the front of the head and also in the face or teeth.
Frequently the face feels tender to tension, particularly just below the eyes beside the nose. You might have a stuffy nose and the pain is often worse when you bend forwards. Acute sinusitis is the kind that comes on fast in conjunction with a cold or abrupt allergy. You may have a temperature and be generating a lot of mucus. Chronic sinusitis may be caused by allergy, by overusing decongestants or with the acute sinusitis that doesn’t settle. The sinuses become chronically infected and the nasal linings chronically swollen. The contents of this uterus may be thick but frequently not infected.
Acute glaucoma can cause severe headaches. In this condition, the pressure inside the eyes goes up suddenly and this causes a surprisingly, very severe headache behind the eye. Even the eyeball can feel really hard to touch, the eye is red, the front part of the eye, or cornea, can seem cloudy and the eyesight is generally blurred.
What Types of Headaches are Dangerous or Serious?
All headaches are unpleasant and some, such as headache from medication abuse, are serious in the sense that if not treated correctly they might never go away. But a few headaches are indications of serious underlying issues. These are uncommon, in many cases very rare. Dangerous headaches often occur suddenly, and also eventually become increasingly worse over time. They are more common in elderly people. They comprise of the following:
Bleeding Around the Brain (Subarachnoid Haemorrhage)
Subarachnoid haemorrhage is a really serious condition which occurs when a tiny blood vessel pops on the surface of the brain. Patients develop a serious headache and stiff neck and may become unconscious. This is a rare cause of acute headache.
Meningitis and Brain Infections
Meningitis is infection of the tissues around and on the surface of the brain and encephalitis is infection of the brain itself. Brain infections can be caused by germs called bacteria, viruses or parasites and they are thankfully rare. They cause a severe, disabling headache. Normally, patients may feel sick or vomit and can’t bear bright lights, something known as photophobia. Often they have a rigid neck, too stiff for your physician to have the ability to bend the head down so that the chin touches the chest, even in the event that you attempt to relax. Patients are generally also unwell, experiencing hot, sweaty and overall sick sensations.
Giant Cell Arteritis (Temporal Arteritis)
Giant cell arteritis (temporal arteritis) is, generally, just seen in people over the age of 50. It is due to swelling, or inflammation, of the arteries at the temples and behind the eye. It causes a headache behind the forehead, also referred to as a sinus headache. Typically the blood vessels at the forehead are tender and individuals detect pain from the scalp when they comb their own hair. Frequently the pain gets worse with chewing. Temporal arteritis is severe because if it’s not treated it can cause sudden loss of eyesight. Treatment is with a course of steroids. The need to keep these steroids is generally monitored by the GP through blood tests, and they are typically needed for several months.
Brain Tumors
Brain tumors are a very uncommon cause of headache, although most patients with long-term, severe or persistent headaches start to worry that this might be the reason. Brain tumors can lead to headaches. Usually the aggravation of brain tumors exists on waking in the morning, is worse on sitting up, and becoming steadily worse in the day to day, never easing and never disappearing. It can sometimes be worse on coughing and sneezing, as may sinus headaches and migraines.
When Should I Worry About a Headache?
Most headaches do not have a serious underlying cause. However, healthcare professionals are trained to ask you about the signs and symptoms that might suggest your headache needs further diagnosis, just to make certain it’s nothing serious.
The things which would suggest to your physician and nurse that your headache may need additional evaluation include the following. They don’t mean that your headache is severe or sinister, but they imply that the healthcare professional may wish to do some additional evaluations to make sure if:
You have had a substantial head injury in the previous three months.
Your headaches are worsening and accompanied with high temperature or fever.
Your headaches begin extremely unexpectedly.
You’ve developed problems with speech and balance as well as headache.
You’ve developed problems with your memory or changes in your behavior or personality in addition to headache.
You’re confused or muddled along with your headache.
Your headache started when you coughed, sneezed or strained.
Your headache is much worse when you sit or stand.
Your headache is associated with red or painful eyes.
Your headaches are not like anything you’ve ever experienced before.
You have unexplained nausea together with the aggravation.
You have low immunity, for instance, when you have HIV, or are about oral steroid medicine or immune suppressing drugs.
You have or have had a type of cancer that can spread throughout the body.
Dr. Alex Jimenez’s Insight
Headaches are extremely common health issues which affect a wide range of the population around the world. Although frequent, a headache which is described to be like no other ever experienced before, may often become a concern. There are several types of headaches which can be caused by a variety of injuries and/or underlying conditions. As a healthcare professional, it’s essential to be able to determine between sinister or dangerous types of headaches and benign types of headaches, in order to decide the best treatment approach. By properly diagnosing the source of a patient’s headaches, both benign and sinister types of headaches can be treated accordingly.
Overview
Many headaches, whilst unpleasant, are harmless and react to a variety of treatments, including chiropractic care. Migraine, tension headaches and medication-overuse headaches are very common. The majority of the populace will experience one or more of these. Working out exactly the underlying cause of any headaches through discussion with your doctor is often the best method to resolve them. It is possible to develop a persistent or chronic and constant headache through taking drugs and/or medications that you took to get rid of your headache. Your physician can support you through the practice of quitting painkillers when that is the case.
Headaches are, quite infrequently, an indication of a serious or sinister underlying illness, and many headaches go away on their own.
If you have a headache which is uncommon for you then you need to discuss it with your doctor. You should also speak to your doctor about headaches which are particularly severe or that affect your regular activities, those that are associated with other symptoms, such as tingling or weakness, and those which make your own scalp tender, especially if you’re over 50 years old. Finally, always speak to a healthcare professional when you have an unremitting morning headache which is present for at least three days or is becoming gradually worse.
Remember that headaches are not as likely to occur in people who:
Handle their anxiety levels well.
Eat a balanced, regular diet.
Take balanced routine exercise.
Focus on posture and core muscles.
Sleep on two pillows or fewer.
Drink loads of water.
Have plenty of sleep.
Anything that you can do to enhance one or more of these aspects of your life will improve your health and well-being and cut back the number of headaches you experience. Make sure to seek the appropriate medical attention from a qualified and experienced healthcare professional in the event of a severe headache unlike anything you’ve ever experienced before. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Suffer Migraines: If you�ve ever had a migraine you know that it�s more than just a headache. The debilitating pain can be accompanied by nausea and other symptoms � and it�s more common than you may think. Research shows that in every four American households, one person is a migraine sufferer. In fact, 12 percent of the U.S. population suffers from migraines, including children. This means migraines affect more people that asthma and diabetes combined.
It is estimated that 18 percent of women suffer from migraines while 6 percent of men are migraine sufferers. It most commonly affects people who are between the ages of 25 and 55, but even young children have been diagnosed. Migraines can stop you in your tracks, but there are treatments that can help. Chiropractic care has been shown to help ease the pain, intensity, and frequency of migraines.
Suffer From Migraines
What Is A Migraine?
Migraines are vicious headaches that can last several minutes to several hours or even days. It is characterized by intense pulsing or a throbbing sensation that is typically confined to one area of the head. It is often accompanied by vomiting, nausea, and extreme sensitivity to sound and light. The pain can be so severe that you can barely function. Many people find themselves confined to bed in a darkened room, waiting for it to pass.
Many times migraine sufferers report experiencing an aura, or sensory warning symptoms, such as strange smells, blind spots, flashes of light, or tingling in your leg or arm. They also tend to run in families. If one parent is a migraine sufferer the child has a 40 percent chance of having migraines as well. If both parents get migraines that chance jumps to 90 percent. It is the 8th most debilitating illness on a global scale.
For the most part, doctors do not know much about what causes migraines. However, there are some things that have been identified as migraine triggers:
Hormonal changes � at certain times during the month, women experience fluctuations in estrogen which can trigger migraines
Oral contraceptives � medications that change or replace hormones can make headaches worse
Certain foods � processed foods, MSG, salty foods, aged cheeses
Fasting or skipping meals
Aspartame
Alcohol
Stress
Sensory overstimulation
Dehydration
Intense physical exertion
Too much or too little sleep
Medications
How Chiropractic Care Can Help Migraine Sufferers
Many doctors believe that headaches and migraines may be caused by a spine that is out of alignment. When your spine is misaligned your entire body suffers. It can irritate the nerves that run from the brain to the spine causing a headache. Chiropractic adjustments can help relieve the pain of migraines. In fact, many people report a distinct difference after just one session.
A Doctor of Chiropractic will align your spine and work with you to create a wellness plan that includes lifestyle changes and diet. Making changes to your sleep patterns and eliminating certain foods from your diet can help prevent migraines. By creating a whole body wellness program, you and your chiropractor can not only help prevent your migraines, but other health conditions as well.
Your chiropractor may also recommend that you keep a journal to help you pinpoint your own unique migraine triggers. You will record the foods you eat, environmental factors that may affect you, stressors, and sleep patterns, as well as when you have migraines, how long they last, and their severity. By tracking these things, you can determine what may be causing your migraines and make adjustments to your lifestyle, thus preventing them. Incorporating chiropractic care as part of your whole body maintenance, as well as migraine prevention, can help you stave off these headaches so you can get on with your life.
If you or a loved one suffers from migraine headaches, make sure you give us a call. Our Doctor of Chiropractic is here to help!
Headaches can be a real aggravating issue, especially if these begin to occur more frequently. Even more so, headaches can become a bigger problem when the common type of head pain becomes a migraine. Head pain is often a symptom resulting from an underlying injury and/or condition along the cervical spine, or upper back and neck. Fortunately, a variety of treatment methods are available to help treat headaches. Chiropractic care is a well-known alternative treatment option which is commonly recommended for neck pain, headaches and migraines. The purpose of the following research study is to determine the effectiveness of chiropractic spinal manipulative therapy for migraine.
Chiropractic Spinal Manipulative Therapy for Migraine: a Study Protocol of a Single-Blinded Placebo-Controlled Randomised Clinical Trial
Abstract
Introduction
Migraine affects 15% of the population, and has substantial health and socioeconomic costs. Pharmacological management is first-line treatment. However, acute and/or prophylactic medicine might not be tolerated due to side effects or contraindications. Thus, we aim to assess the efficacy of chiropractic spinal manipulative therapy (CSMT) for migraineurs in a single-blinded placebo-controlled randomised clinical trial (RCT).
Method and Analysis
According to the power calculations, 90 participants are needed in the RCT. Participants will be randomised into one of three groups: CSMT, placebo (sham manipulation) and control (usual non-manual management). The RCT consists of three stages: 1?month run-in, 3?months intervention and follow-up analyses at the end of the intervention and 3, 6 and 12?months. The primary end point is migraine frequency, while migraine duration, migraine intensity, headache index (frequency x duration x intensity) and medicine consumption are secondary end points. Primary analysis will assess a change in migraine frequency from baseline to the end of the intervention and follow-up, where the groups CSMT and placebo and CSMT and control will be compared. Owing to two group comparisons, p values below 0.025 will be considered statistically significant. For all secondary end points and analyses, a p value below 0.05 will be used. The results will be presented with the corresponding p values and 95% CIs.
Ethics and Dissemination
The RCT will follow the clinical trial guidelines from the International Headache Society. The Norwegian Regional Committee for Medical Research Ethics and the Norwegian Social Science Data Services have approved the project. Procedure will be conducted according to the declaration of Helsinki. The results will be published at scientific meetings and in peer-reviewed journals.
Trial Registration Number
NCT01741714.
Keywords:Statistics & Research Methods
Strengths and Limitations of this Study
The study will be the first three-armed manual therapy randomised clinical trial (RCT) assessing the efficacy of chiropractic spinal manipulative therapy versus placebo (sham manipulation) and control (continue usual pharmacological management without receiving manual intervention) for migraineurs.
Strong internal validity, since a single chiropractor will conduct all interventions.
The RCT has the potential to provide a non-pharmacological treatment option for migraineurs.
Risk for dropouts is increased due to strict exclusion criteria and 17?months duration of the RCT.
A generally accepted placebo has not been established for manual therapy; thus, there is a risk for unsuccessful blinding, while the investigator who provides the interventions cannot be blinded for obvious reasons.
Background
Migraine is a common health problem with substantial health and socioeconomic costs. On the recent Global Burden of Disease study, migraine was ranked as the third most common condition.[1]
About 15% of the general population have migraine.[2, 3] Migraine is usually unilateral with pulsating and moderate/severe headache which is aggravated by routine physical activity, and is accompanied by photophobia and phonophobia, nausea and sometimes vomiting.[4] Migraine exists in two major forms, migraine without aura and migraine with aura (below). Aura is reversible neurological disturbances of the vision, sensory and/or speech function, occurring prior to the headache. However, intraindividual variations from attack to attack are common.[5, 6] The origin of migraine is debated. The painful impulses may originate from the trigeminal nerve, central and/or peripheral mechanisms.[7, 8] Extracranial pain sensitive structures include the skin, muscles, arteries, periosteum and joints. The skin is sensitive to all usual forms of pain stimuli, while temporal and neck muscles may especially be sources for pain and tenderness in migraine.[9�11] Similarly, the frontal supraorbital, superficial temporal, posterior and occipital arteries are sensitive to pain.[9, 12]
Notes
The International Classification of Headache Disorders-II Diagnostic Criteria for Migraine
Migraine without Aura
A. At least five attacks fulfilling criteria B�D
B. Headache attacks lasting 4�72?h (untreated or unsuccessfully treated)
C. Headache has at least two of the following characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe pain intensity
4. Aggravated by or causing avoidance of routine physical activity
D. During headache at least one of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E. Not attributed to another disorder
Migraine with aura
A. At least two attacks fulfilling criteria B�D
B. Aura consisting of at least one of the following, but no motor weakness:
1. Fully reversible visual symptoms including positive features (ie, flickering lights, spots or lines) and/or negative features (ie, loss of vision). Moderate or severe pain intensity
2. Fully reversible sensory symptoms including positive features (ie, pins and needles) and/or negative features (ie, numbness)
2. At least one aura symptom develops gradually over ?5?min and/or different aura symptoms occur in succession over ?5?min
3. Each symptom lasts ?5 and ?60?min
D. Headache fulfilling criteria B-D for 1.1 Migraine without aura begins during the aura or follows the aura within 60?min
E. Not attributed to another disorder
Pharmacological management is the first treatment option for migraineurs. However, some patients do not tolerate acute and/or prophylactic medicine due to side effects or contraindications due to comorbidity of other diseases or due to a wish to avoid medication for other reasons. The risk of medication overuse due to frequent migraine attacks represents a major health hazard with direct and indirect cost concerns. The prevalence of medication overuse headache (MOH) is 1�2% in the general population,[13�15] that is, about half the population suffering chronic headache (15 headache days or more per month) have MOH.[16] Migraine causes loss of 270 workdays per year per 1000 persons from the general population.[17] This corresponds to about 3700 work years lost per year in Norway due to migraine. The economic cost per migraineur was estimated to be $655 in USA and �579 in Europe per year.[18, 19] Owing to the high prevalence of migraine, the total cost per year was estimated to be $14.4 billion in the USA and �27 billion in the EU countries, Iceland, Norway and Switzerland at that time. Migraine costs more than neurological disorders such as dementia, multiple sclerosis, Parkinson’s disease and stroke.[20] Thus, non-pharmacological treatment options are warranted.
The Diversified technique and the Gonstead method are the two most commonly used chiropractic manipulative treatment modalities in the profession, used by 91% and 59%, respectively,[21, 22] along with other manual and non-manual interventions, that is, soft tissue techniques, spinal and peripheral mobilisation, rehabilitation, postural corrections and exercises as well as general nutrition and dietetic advice.
A few spinal manipulative therapy (SMT) randomised controlled trials (RCTs) using the Diversified technique have been conducted for migraine, suggesting an effect on migraine frequency, migraine duration, migraine intensity and medicine consumption.[23�26] However, common for previous RCTs are the methodological shortcomings such as inaccurate headache diagnosis, that is, questionnaire diagnoses used are imprecise,[27] inadequate or no randomisation procedure, lack of placebo group, and primary and secondary end points not prespecified.[28�31] In addition, previous RCTs did not consequently adhere to the recommended clinical guidelines from the International Headache Society (IHS).[32, 33] At present, no RCTs have applied the Gonstead chiropractic SMT (CSMT) method. Thus, considering the methodological shortcomings in previous RCTs, a clinical placebo-controlled RCT with improved methodological quality remains to be conducted for migraine.
The SMT mechanism of action on migraine is unknown. It is argued that migraine might originate from a complexity of nociceptive afferent responses involving the upper cervical spine (C1, C2 and C3), leading to a hypersensitivity state of the trigeminal pathway conveying sensory information for the face and much of the head.[34, 35] Research has thus suggested that SMT may stimulate neural inhibitory systems at different spinal cord levels, and might activate various central descending inhibitory pathways.[36�40] However, although the proposed physiological mechanisms are not fully understood, there are most likely additional unexplored mechanisms which could explain the effect SMT has on mechanical pain sensitisation.
The objective of this study is to assess the efficacy of CSMT versus placebo (sham manipulation) and controls (continue usual pharmacological management without receiving manual intervention) for migraineurs in an RCT.
Method and Design
This is a single-blinded placebo-controlled RCT with three parallel groups (CSMT, placebo and control). Our primary hypothesis is that CSMT gives at least 25% reduction in the average number of migraine days per month (30?days/month) as compared to placebo and control from baseline to the end of intervention, and we expect the same reduction to be maintained at 3, 6 and 12?months follow-up. If the CSMT treatment is effective, it will be offered to participants who received placebo or control after study completion, that is, after 12?months follow-up. The study will adhere to the recommended clinical trial guidelines from the IHS,32 33 and the methodological CONSORT and SPIRIT guidelines.[41, 42]
Patient Population
Participants will be recruited in the period January to September 2013 through the Akershus University Hospital, through general practitioners and media advertisement, that is, posters with general information will be put up at general practitioners� offices along with oral information in the Akershus and Oslo counties, Norway. Participants will receive posted information about the project followed by a short telephone interview. Those recruited from the general practitioners� offices will have to contact the clinical investigator whose contact details have been provided on the posters in order to obtain extensive information about the study.
Eligible participants are between 18 and 70?years of age and have at least one migraine attack per month. Participants are diagnosed according to the diagnostic criteria of the International Classification of Headache Disorders (ICHD-II) by a neurologist at the Akershus University Hospital.[43] They are only allowed to have co-occurrence of tension-type headache and not other primary headaches.
Exclusion criteria are contraindication to SMT, spinal radiculopathy, pregnancy, depression and CSMT within the previous 12?months. Participants whom during the RCT receive any manual interventions by physiotherapists, chiropractors, osteopaths or other health professionals to treat musculoskeletal pain and disability, including massage therapy, joint mobilisation and manipulation,[44] changed their prophylactic headache medicine or pregnancy will be withdrawn from the study at that time and be regarded as dropouts. They are allowed to continue and change their usual acute migraine medication throughout the trial.
In response to initial contact, participants fulfilling the inclusion criteria will be invited to further assessment by the chiropractic investigator. The assessment includes an interview and a physical examination with special emphasis on the whole spinal column. Oral and written information about the project will be provided in advance and oral and written consent will be obtained from all accepted participants during the interview and by the clinical investigator. In accordance with good clinical practice, all patients will be informed about the harms and benefits as well as possible adverse reactions of the intervention primarily including local tenderness and tiredness on the treatment day. No serious adverse events have been reported for the chiropractic Gonstead method.[45, 46] Participants randomised into active or placebo interventions will undergo a full spine radiographic examination and be scheduled for 12 intervention sessions. The control group will not be exposed to this assessment.
Clinical RCT
The clinical RCT consists of a 1?month run-in and 3?months intervention. Time profile will be assessed from baseline to the end of follow-up for all end points (Figure 1).
The participants will fill in a validated diagnostic paper headache diary 1?month prior to intervention which will be used as baseline data for all participants.[47, 48] The validated diary includes questions directly related to the primary and secondary end points. X-rays will be taken in standing position in the anterioposterior and lateral planes of the entire spine. The X-rays will be assessed by the chiropractic investigator.
Randomisation
Prepared sealed lots with the three interventions, that is, active treatment, placebo and the control group, will be subdivided into four subgroups by age and gender, that is, 18�39 and 40�70?years of age and men and women, respectively. Participants will be equally allocated to the three groups by allowing the participant to draw one lot only. The block randomisation will be administrated by an external trained party with no involvement from the clinical investigator.
Intervention
Active treatment consists of CSMT using the Gonstead method,[21] that is, a specific contact, high-velocity, low-amplitude, short-lever spinal with no postadjustment recoil directed to spinal biomechanical dysfunction (full spine approach) as diagnosed by standard chiropractic tests.
The placebo intervention consists of sham manipulation, that is, a broad non-specific contact, low-velocity, low-amplitude sham push manoeuvre in a non-intentional and non-therapeutic directional line. All the non-therapeutic contacts will be performed outside the spinal column with adequate joint slack and without soft tissue pretension so that no joint cavitations occur. In some sessions, the participant lay either prone on a Zenith 2010 HYLO bench with the investigator standing at the participant’s right side with his left palm placed on the participant’s right lateral scapular edge with the other hand reinforcing. In other sessions, the investigator will stand at the participant’s left side and place his right palm over the participant’s left scapular edge with the left hand reinforcing, delivering a non-intentional lateral push manoeuvre. Alternatively, the participant lay in the same side posture position as the active treatment group with the bottom leg straight and the top leg flexed with the top leg’s ankle resting on the bottom leg’s knee fold, in preparation for a side posture push move, which will be delivered as a non-intentional push in the gluteal region. The sham manipulation alternatives will be equally interchanged among the placebo participants according to protocol during the 12-week treatment period to strengthen the study validity. The active and the placebo groups will receive the same structural and motion assessment prior to and after each intervention. No additional cointerventions or advice will be given to participants during the trial period. The treatment period will include 12 consultations, that is, twice per week in the first 3?weeks followed by once a week in the next 2?weeks and once every second week until 12?weeks are reached. Fifteen minutes will be allocated per consultation for each participant. All interventions will be conducted at the Akershus University Hospital and administered by an experienced chiropractor (AC).
The control group will continue usual care, that is, pharmacological management without receiving manual intervention by the clinical investigator. The same exclusion criteria apply for the control group during the whole study period.
Blinding
After each treatment session, the participants who receive active or placebo intervention will complete a de-blinding questionnaire administrated by an external trained independent party with no involvement from the clinical investigator, that is, providing a dichotomous �yes� or �no� answer as to whether active treatment was received. This response was followed by a second question regarding how certain they were that active treatment was received on a 0�10 numeric rating scale (NRS), where 0 represents absolutely uncertain and 10 represents absolutely certainty. The control group and the clinical investigator can for obvious reasons not be blinded.[49, 50]
Follow-Up
Follow-up analysis will be conducted on the end points measured after the end of intervention and at 3, 6 and 12?months follow-up. During this period, all participants will continue to fill in a diagnostic paper headache diary and return it on a monthly basis. In the case of unreturned diary or missing values in the diary, the participants will be contacted immediately on detection to minimise recall bias. Participants will be contacted by phone to secure compliance.
Primary and Secondary End Points
The primary and secondary end points are listed below. The end points adhere to the recommended IHS clinical trial guidelines.[32, 33] We define number of migraine days as the primary end point and expect at least a 25% reduction in average number of days from baseline to the end of intervention, with the same level of reduction being maintained at follow-up. On the basis of previous reviews on migraine, a 25% reduction is considered to be a conservative estimate.[30] A 25% reduction is also expected in secondary end points from baseline to the end of intervention, retaining at follow-up for migraine duration, migraine intensity and headache index, where the index is calculated as number of migraine days (30?days)�average migraine duration (hours per day)�average intensity (0�10 NRS). A 50% reduction in medication consumption from baseline to the end of intervention and to follow-up is expected.
Notes
Primary and Secondary End Points
Primary End Points
1. Number of migraine days in active treatment versus placebo group.
2. Number of migraine days in active treatment versus control group.
Secondary End Points
3. Migraine duration in hours in active treatment versus placebo group.
4. Migraine duration in hours in active treatment versus control group.
5. Self-reported VAS in active treatment versus placebo group.
6. Self-reported VAS in active treatment versus control group.
7. Headache index (frequency x duration x intensity) in active treatment versus placebo group.
8. Headache index in active treatment versus control group.
9. Headache medication dosage in active treatment versus placebo group.
10. Headache medication dosage in active treatment versus control group.
*The data analysis is based on the run-in period versus end of intervention. Point 11�40 will be duplicate of point 1�10 above at 3, 6 and 12?months follow-up, respectively.
Data Processing
A flow chart of the participants is shown in Figure 2. Baseline demographic and clinical characteristics will be tabulated as means and SDs for continuous variables and proportions and percentages for categorical variables. Each of three groups will be described separately. Primary and secondary end points will be presented by suitable descriptive statistics in each group and for each time point. Normality of end points will be assessed graphically and transformation will be considered if necessary.
Change in primary and secondary end points from baseline to the end of intervention and to follow-up will be compared between the active and placebo groups and the active and control groups. The null hypothesis states that there is no significant difference between the groups in average change, while the alternative hypothesis states that a difference of at least 25% exists.
Owing to the follow-up period, repeated recordings of primary and secondary end points will be available, and analyses of trend in primary and secondary end points will be of main interest. Intra-individual correlations (cluster effect) are likely to be present in data with repeated measurements. Cluster effect will thus be assessed by calculating intraclass correlation coefficient quantifying the proportion of total variation attributable to the intraindividual variations. The trend in end points will be assessed by a linear regression model for longitudinal data (linear mixed model) to correctly account for the possible cluster effect. The linear mixed model handles unbalanced data, enabling all available information from randomised patients to be included, as well as from dropouts. Regression models with fixed effects for time component and group allocation as well as the interaction between the two will be estimated. The interaction will quantify possible differences between groups regarding time trend in the end points and serve as an omnibus test. Random effects for patients will be included to adjust the estimates for intraindividual correlations. Random slopes will be considered. The linear mixed models will be estimated by the SAS PROC MIXED procedure. The two pairwise comparisons will be performed by deriving individual time point contrasts within each group with the corresponding p values and 95% CIs.
Both per-protocol and intention-to-treat analyses will be conducted if relevant. All analyses will be performed by a statistician, blinded for group allocation and participants. All adverse effects will also be registered and presented. Participants who experience any sort of adverse effects during the trial period will be entitled to call the clinical investigator on the project cell phone. The data will be analysed with SPSS V.22 and SAS V.9.3. Owing to two group comparisons in the primary end point, p values below 0.025 will be considered statistically significant. For all secondary end points and analyses, a significance level of 0.05 will be used. Missing values might appear in incomplete interview questionnaires, incomplete headache diaries, missed intervention sessions and/or due to dropouts. The pattern of missingness will be assessed and missing values handled adequately.
Power Calculation
Sample size calculations are based on the results in a recently published group comparison study on topiramate.[51] We hypothesise that the average difference in reduction of number of days with migraine per month between the active and the placebo groups is 2.5?days. The same difference is assumed between the active and control groups. SD for reduction in each group is assumed to be equal to 2.5. Under the assumption of, on average, 10 migraine days per month at baseline in each group and no change in the placebo or control group during the study, 2.5?days reduction corresponds to a reduction by 25%. Since primary analysis includes two group comparisons, we set a significance level at 0.025. A sample size of 20 patients is required in each group to detect a statistically significant average difference in reduction of 25% with 80% power. To allow for dropouts, the investigators plan to recruit 120 participants.
Dr. Alex Jimenez’s Insight
“I’ve been recommended to seek chiropractic care for my migraine-type headaches. Is chiropractic spinal manipulative therapy effective for migraine?”�Many different types of treatment options can be utilized to effectively treat migraine, however, chiropractic care is one of the most popular treatment approaches for naturally treating migraine. Chiropractic spinal manipulative therapy�is the traditional high-velocity low-amplitude (HVLA) thrust. Also known as spinal manipulation, a chiropractor performs this chiropractic technique by applying a controlled sudden force to a joint while the body is positioned in a specific way. According to the following article, chiropractic spinal manipulative therapy can effectively help treat migraine.
Discussion
Methodological Considerations
Current SMT RCTs on migraine suggest treatment efficacy regarding migraine frequency, duration and intensity. However, a firm conclusion requires clinical single-blinded placebo-controlled RCTs with few methodological shortcomings.[30] Such studies should adhere to the recommended IHS clinical trial guidelines with migraine frequency as the primary end point and migraine duration, migraine intensity, headache index and medication consumption as secondary end points.[32, 33] The headache index, as well as a combination of frequency, duration and intensity, gives an indication of the total level of suffering. Despite the lack of consensus, the headache index has been recommended as an accepted standard secondary end point.[33, 52, 53] The primary and secondary end points will be collected prospectively in a validated diagnostic headache diary for all participants in order to minimise recall bias.[47, 48] To the best of our knowledge, this is the first prospective manual therapy in a three-armed single-blinded placebo-controlled RCT to be conducted for migraine. The study design adheres to the recommendations for pharmacological RCTs as far as possible. RCTs that include a placebo group and a control group are advantageous to pragmatic RCTs that compare two active treatment arms. RCTs also provide the best approach for producing safety as well as efficacy data.
Unsuccessful blinding is a possible risk to the RCT. Blinding is often difficult as there is no single validated standardised chiropractic sham intervention which can be used as a control group for this date. It is, however, necessary to include a placebo group in order to produce a true net effect of the active intervention. Consensus about an appropriate placebo for a clinical trial of SMT among experts representing clinicians and academics has, however, not been reached.[54] No previous studies have, to the best of our knowledge, validated a successful blinding of a CSMT clinical trial with multiple treatment sessions. We intend to minimise this risk by following the proposed protocol for the placebo group.
The placebo response is furthermore high in pharmacological and assumed similarly high for non-pharmacological clinical studies; however, it might even be higher in manual therapy RCTs were attention and physical contact is involved.[55] Similarly, a natural concern with regard to attention bias will be involved for the control group as it is not being seen by anyone or not seen as much by the clinical investigator as the other two groups.
There are always risks for dropouts due to various reasons. Since the trial duration is 17?months with a 12?month follow-up period, the risk for loss to follow-up is thus enhanced. Co-occurrence of other manual intervention during the trial period is another possible risk, as those who receive manipulation or other manual physical treatments elsewhere during the trial period will be withdrawn from the study and regarded as dropouts at the time of violation.
The external validity of the RCT might be a weakness as there is only one investigator. However, we found that advantageous to multiple investigators, in order to provide similar information to participants in all three groups and manual intervention in the CSMT and the placebo groups. Thus, we intend to eliminate inter-investigator variability which might be present if there are two or more investigators. Although the Gonstead method is the second most commonly used technique among chiropractors, we do not see an issue of concern when it comes to generalisability and external validity. Furthermore, the block randomisation procedure will provide a homogeneous sample across the three groups.
The internal validity is, however, strong by having one treating clinician. It reduces the risk of potential selection, information and experimental biases. Furthermore, the diagnosis of all participants is performed by experienced neurologists and not by questionnaires. A direct interview has higher sensitivity and specificity as compared to a questionnaire.[27] Individual motivational factors which can influence a participant’s perception and personal preferences when treating are both reduced by having one investigator. In addition, the internal validity is further strengthened by a concealed validated randomisation procedure. Since age and genders may play a role in migraine, block randomisation was found necessary to balance arms by age and gender in order to reduce possible age-related and/or gender-related bias.
X-rays demonstrating loss of cervical lordosis as a possible cause for migraine.
Conducting X-rays prior to the active and placebo interventions was found to be applicable in order to visualise posture, joint and disc integrity.[56, 57] Since the total X-ray radiation dose varies from 0.2�0.8?mSv, the radiation exposure was considered low.[58, 59] X-ray assessments were also found to be necessary in order to determine if full spine X-rays are useful in future studies or not.
Since we are unaware of the mechanisms of possible efficacy, and both spinal cord and central descending inhibitory pathways have been postulated, we see no reasons to exclude a full spine treatment approach for the intervention group. It has furthermore been postulated that pain in different spinal regions should not be regarded as separate disorders but rather as a single entity.[60] Similarly, including a full spine approach limits the differentiations between the CSMT and the placebo groups. Thus, it might strengthen the likelihood of successful blinding in the placebo group being achieved. In addition, all the placebo contacts will be performed outside the spinal column, thus minimising a possible spinal cord afferent input.
Innovative and Scientific Value
This RCT will highlight and validate the Gonstead CSMT for migraineurs, which has not previously been studied. If CSMT proves to be effective, it will provide a non-pharmacological treatment option. This is especially important as some migraineurs do not have efficacy of prescript acute and/or prophylactic medications, while others have non-tolerable side effects or comorbidity of other diseases that contradict medication while others wish to avoid medication for various reasons. Thus, if CSMT works, it can really have an impact on migraine treatment. The study also bridges cooperation between chiropractors and physicians, which is important in order to make healthcare more efficient. Finally, our method might be applied in future chiropractic and other manual therapy RCTs on headache.
Ethics and Dissemination
Ethics
The study has been approved by the Norwegian Regional Committee for Medical Research Ethics (REK) (2010/1639/REK) and the Norwegian Social Science Data Services (11�77). The declaration of Helsinki is otherwise followed. All data will be anonymised while participants must give oral and written informed consent. Insurance is provided through �The Norwegian System of Compensation to Patients� (NPE), which is an independent national body set up to process compensation claims from patients who have suffered an injury as a result of treatment under the Norwegian health service. A stopping rule was defined for withdrawing participants from this study in accordance with recommendations in the CONSORT extension for Better Reporting of Harms.[61] If a participant reports to their chiropractor or research staff a severe adverse event, he or she will be withdrawn from the study and referred to their general practitioner or hospital emergency department depending on the nature of the event. The final data set will be available to the clinical investigator (AC), the independent and blinded statistician (JSB) and Study Director (MBR). Data will be stored in a locked cabinet at the Research Centre, Akershus University Hospital, Norway, for 5?years.
Dissemination
This project is due for completion 3?years after the start. Results will be published in peer-reviewed international scientific journals in accordance with the CONSORT 2010 Statement. Positive, negative, as well as inconclusive results will be published. In addition, a written lay summary of the results will be available to study participants on request. All authors should qualify for authorship according to the International Committee of Medical Journal Editors, 1997. Each author should have participated sufficiently in the work to take public responsibility for the content. The final decision on the order of authorship will be decided when the project has been finalised. The results from the study may, moreover, be presented as posters or oral presentations at national and/or international conferences.
Acknowledgments
Akershus University Hospital kindly provided research facilities. Chiropractor Clinic1, Oslo, Norway, performed X-ray assessments.
Footnotes
Contributors: AC and PJT had the original idea for the study. AC and MBR obtained funding. MBR planned the overall design. AC prepared the initial draft and PJT commented on the final version of the research protocol. JSB performed all the statistical analyses. AC, JSB, PJT and MBR were involved in the interpretation and assisted in the revision and preparation of the manuscript. All authors have read and approved the final manuscript.
Funding: The study has received funding from Extrastiftelsen (grant number: 2829002), the Norwegian Chiropractic Association (grant number: 2829001), Akershus University Hospital (grant number: N/A) and University of Oslo in Norway (grant number: N/A).
Competing interests: None declared.
Patient consent: Obtained.
Ethics approval: The Norwegian Regional Committee for Medical Research Ethics approved the project (ID of the approval: 2010/1639/REK).
Provenance and peer review: Not commissioned; externally peer reviewed.
A Randomized Controlled Trial of Chiropractic Spinal Manipulative Therapy for Migraine
Abstract
Objective: To assess the efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine.
Design: A randomized controlled trial of 6 months’ duration. The trial consisted of 3 stages: 2 months of data collection (before treatment), 2 months of treatment, and a further 2 months of data collection (after treatment). Comparison of outcomes to the initial baseline factors was made at the end of the 6 months for both an SMT group and a control group.
Setting: Chiropractic Research Center of Macquarie University.
Participants: One hundred twenty-seven volunteers between the ages of 10 and 70 years were recruited through media advertising. The diagnosis of migraine was made on the basis of the International Headache Society standard, with a minimum of at least one migraine per month.
Interventions: Two months of chiropractic SMT (diversified technique) at vertebral fixations determined by the practitioner (maximum of 16 treatments).
Main Outcome Measures: Participants completed standard headache diaries during the entire trial noting the frequency, intensity (visual analogue score), duration, disability, associated symptoms, and use of medication for each migraine episode.
Results: The average response of the treatment group (n = 83) showed statistically significant improvement in migraine frequency (P < .005), duration (P < .01), disability (P < .05), and medication use (P< .001) when compared with the control group (n = 40). Four persons failed to complete the trial because of a variety of causes, including change in residence, a motor vehicle accident, and increased migraine frequency. Expressed in other terms, 22% of participants reported more than a 90% reduction of migraines as a consequence of the 2 months of SMT. Approximately 50% more participants reported significant improvement in the morbidity of each episode.
Conclusion: The results of this study support previous results showing that some people report significant improvement in migraines after chiropractic SMT. A high percentage (>80%) of participants reported stress as a major factor for their migraines. It appears probable that chiropractic care has an effect on the physical conditions related to stress and that in these people the effects of the migraine are reduced.
In conclusion, chiropractic spinal manipulative therapy can be used effectively to help treat migraine, according to the research study. Furthermore, chiropractic care improved the individual’s overall health and wellness. The well-being of the human body as a whole is believed to be one of the biggest factors as to why chiropractic care is effective for migraine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Vos T, Flaxman AD, Naghavi M et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990�2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2163�96. doi:10.1016/S0140-6736(12)61729-2[PubMed]
2. Russell MB, Kristiansen HA, Saltyte-Benth J et al. A cross-sectional population-based survey of migraine and headache in 21,177 Norwegians: the Akershus sleep apnea project. J Headache Pain 2008;9:339�47. doi:10.1007/s10194-008-0077-z[PMC free article][PubMed]
3. Steiner TJ, Stovner LJ, Katsarava Z et al. The impact of headache in Europe: principal results of the Eurolight project. J Headache Pain 2014;15:31 doi:10.1186/1129-2377-15-31[PMC free article][PubMed]
4. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013;33:629�808. doi:10.1177/0333102413485658[PubMed]
5. Russell MB, Iversen HK, Olesen J. Improved description of the migraine aura by a diagnostic aura diary. Cephalalgia 1994;14:107�17. doi:10.1046/j.1468-2982.1994.1402107.x[PubMed]
6. Russell MB, Olesen J. A nosographic analysis of the migraine aura in a general population. Brain 1996;119(Pt 2):355�61. doi:10.1093/brain/119.2.355[PubMed]
7. Olesen J, Burstein R, Ashina M et al. Origin of pain in migraine: evidence for peripheral sensitisation. Lancet Neurol 2009;8:679�90. doi:10.1016/S1474-4422(09)70090-0[PubMed]
8. Amin FM, Asghar MS, Hougaard A et al. Magnetic resonance angiography of intracranial and extracranial arteries in patients with spontaneous migraine without aura: a cross-sectional study. Lancet Neurol 2013;12:454�61. doi:10.1016/S1474-4422(13)70067-X[PubMed]
9. Wolff HGF. Headache and other head pain. 2nd edn Oxford: Oxford University Press, 1963.
10. Jensen K. Extracranial blood flow, pain and tenderness in migraine. Clinical and experimental studies. Acta Neurol Scand Suppl 1993;147:1�8. doi:10.1111/j.1748-1716.1993.tb09466.x[PubMed]
11. Svensson P, Ashina M. Human studies of experimental pain from muscles. In: Olesen J, Tfelt-Hansen P, Welch KMA et al., eds Headache. 3rd edn Lippincott Williams & Wilkins, 2006:627�35.
12. Ray BS, Wolff HG. Experimental studies on headache. Pain sensitive structures of the head and their significance in headache. Arch Surg 1940;41:813�56. doi:10.1001/archsurg.1940.01210040002001
13. Grande RB, Aaseth K, Gulbrandsen P et al. Prevalence of primary chronic headache in a population-based sample of 30- to 44-year-old persons. The Akershus study of chronic headache. Neuroepidemiology 2008;30:76�83. doi:10.1159/000116244[PubMed]
14. Aaseth K, Grande RB, Kvaerner KJ et al. Prevalence of secondary chronic headaches in a population-based sample of 30�44-year-old persons. The Akershus study of chronic headache. Cephalalgia 2008;28:705�13. doi:10.1111/j.1468-2982.2008.01577.x[PubMed]
16. Lundqvist C, Grande RB, Aaseth K et al. Dependence scores predict prognosis of medication overuse headache: a prospective cohort from the Akershus study of chronic headache. Pain 2012;153:682�6. doi:10.1016/j.pain.2011.12.008[PubMed]
17. Rasmussen BK, Jensen R, Olesen J. Impact of headache on sickness absence and utilisation of medical services: a Danish population study. J Epidemiol Community Health 1992;46:443�6. doi:10.1136/jech.46.4.443[PMC free article][PubMed]
18. Hu XH, Markson LE, Lipton RB et al. Burden of migraine in the United States: disability and economic costs. Arch Intern Med 1999;159:813�18. doi:10.1001/archinte.159.8.813[PubMed]
20. Andlin-Sobocki P, Jonsson B, Wittchen HU et al. Cost of disorders of the brain in Europe. Eur J Neurol 2005;12(Suppl 1):1�27. doi:10.1111/j.1468-1331.2005.01202.x[PubMed]
24. Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust NZ J Med 1980;10:192�8. doi:10.1111/j.1445-5994.1980.tb03712.x[PubMed]
25. Nelson CF, Bronfort G, Evans R et al. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther 1998;21:511�19. [PubMed]
26. Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther 2000;23:91�5. doi:10.1016/S0161-4754(00)90073-3[PubMed]
28. Vernon HT. The effectiveness of chiropractic manipulation in the treatment of headache: an exploration in the literature. J Manipulative Physiol Ther 1995;18:611�17. [PubMed]
29. Fernandez-de-las-Penas C, Alonso-Blanco C, San-Roman J et al. Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. J Orthop Sports Phys Ther 2006;36:160�9. doi:10.2519/jospt.2006.36.3.160[PubMed]
31. Chaibi A, Russell MB. Manual therapies for primary chronic headaches: a systematic review of randomized controlled trials. J Headache Pain 2014;15:67 doi:10.1186/1129-2377-15-67[PMC free article][PubMed]
32. Tfelt-Hansen P, Block G, Dahlof C et al. International Headache Society Clinical Trial Subcommittee. Guidelines for controlled trials of drugs in migraine: second edition. Cephalalgia 2000;20:765�86. doi:10.1046/j.1468-2982.2000.00117.x[PubMed]
33. Silberstein S, Tfelt-Hansen P, Dodick DW et al. , Task Force of the International Headache Society Clinical Trial Subcommittee . Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults. Cephalalgia 2008;28:484�95. doi:10.1111/j.1468-2982.2008.01555.x[PubMed]
34. Kerr FW. Central relationships of trigeminal and cervical primary afferents in the spinal cord and medulla. Brain Res 1972;43:561�72. doi:10.1016/0006-8993(72)90408-8[PubMed]
36. McLain RF, Pickar JG. Mechanoreceptor endings in human thoracic and lumbar facet joints. Spine (Phila Pa 1976) 1998;23:168�73. doi:10.1097/00007632-199801150-00004[PubMed]
37. Vernon H. Qualitative review of studies of manipulation-induced hypoalgesia. J Manipulative Physiol Ther 2000;23:134�8. doi:10.1016/S0161-4754(00)90084-8[PubMed]
38. Vicenzino B, Paungmali A, Buratowski S et al. Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia. Man Ther 2001;6:205�12. doi:10.1054/math.2001.0411[PubMed]
39. Boal RW, Gillette RG. Central neuronal plasticity, low back pain and spinal manipulative therapy. J Manipulative Physiol Ther 2004;27:314�26. doi:10.1016/j.jmpt.2004.04.005[PubMed]
40. De Camargo VM, Alburquerque-Sendin F, Berzin F et al. Immediate effects on electromyographic activity and pressure pain thresholds after a cervical manipulation in mechanical neck pain: a randomized controlled trial. J Manipulative Physiol Ther 2011;34:211�20. doi:10.1016/j.jmpt.2011.02.002[PubMed]
41. Moher D, Hopewell S, Schulz KF et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c869 doi:10.1136/bmj.c869[PMC free article][PubMed]
42. Hoffmann TC, Glasziou PP, Boutron I et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348:g1687 doi:10.1136/bmj.g1687[PubMed]
43. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004;24(Suppl 1):9�10. doi:10.1111/j.1468-2982.2003.00824.x[PubMed]
44. French HP, Brennan A, White B et al. Manual therapy for osteoarthritis of the hip or knee – a systematic review. Man Ther 2011;16:109�17. doi:10.1016/j.math.2010.10.011[PubMed]
45. Cassidy JD, Boyle E, Cote P et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine (Phila Pa 1976) 2008;33(4Suppl):S176�S83. doi:10.1097/BRS.0b013e3181644600[PubMed]
47. Russell MB, Rasmussen BK, Brennum J et al. Presentation of a new instrument: the diagnostic headache diary. Cephalalgia 1992;12:369�74. doi:10.1111/j.1468-2982.1992.00369.x[PubMed]
48. Lundqvist C, Benth JS, Grande RB et al. A vertical VAS is a valid instrument for monitoring headache pain intensity. Cephalalgia 2009;29:1034�41. doi:10.1111/j.1468-2982.2008.01833.x[PubMed]
49. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials 2004;25:143�56. doi:10.1016/j.cct.2003.10.016[PubMed]
51. Silberstein SD, Neto W, Schmitt J et al. Topiramate in migraine prevention: results of a large controlled trial. Arch Neurol 2004;61:490�5. doi:10.1001/archneur.61.4.490[PubMed]
52. Bendtsen L, Jensen R, Olesen J. A non-selective (amitriptyline), but not a selective (citalopram), serotonin reuptake inhibitor is effective in the prophylactic treatment of chronic tension-type headache. J Neurol Neurosurg Psychiatry 1996;61:285�90. doi:10.1136/jnnp.61.3.285[PMC free article][PubMed]
53. Hagen K, Albretsen C, Vilming ST et al. Management of medication overuse headache: 1-year randomized multicentre open-label trial. Cephalalgia 2009;29:221�32. doi:10.1111/j.1468-2982.2008.01711.x[PubMed]
54. Hancock MJ, Maher CG, Latimer J et al. Selecting an appropriate placebo for a trial of spinal manipulative therapy. Aust J Physiother 2006;52:135�8. doi:10.1016/S0004-9514(06)70049-6[PubMed]
55. Meissner K, Fassler M, Rucker G et al. Differential Effectiveness of Placebo Treatments: A Systematic Review of Migraine Prophylaxis. JAMA Inter Med 2013;173:1941�51. doi:10.1001/jamainternmed.2013.10391[PubMed]
56. Taylor JA. Full-spine radiography: a review. J Manipulative Physiol Ther 1993;16:460�74. [PubMed]
57. International Chiropractic Assocoation Practicing Chiropractors� Committee on Radiology Protocols (PCCRP) for biomechanical assessment of spinal subluxation in chiropractic clinical practice. Secondary International Chiropractic Assocoation Practicing Chiropractors� Committee on Radiology Protocols (PCCRP) for biomechanical assessment of spinal subluxation in chiropractic clinical practice 2009. www.pccrp.org/
58. Cracknell DM, Bull PW. Organ dosimetry in spinal radiography: a comparison of 3-region sectional and full-spine techniques. Chiropr J Austr 2006;36:33�9.
59. Borretzen I, Lysdahl KB, Olerud HM. Diagnostic radiology in Norway trends in examination frequency and collective effective dose. Radiat Prot Dosimetry 2007;124:339�47. doi:10.1093/rpd/ncm204[PubMed]
60. Leboeuf-Yde C, Fejer R, Nielsen J et al. Pain in the three spinal regions: the same disorder? Data from a population-based sample of 34,902 Danish adults. Chiropr Man Ther 2012;20:11 doi:10.1186/2045-709X-20-11[PMC free article][PubMed]
61. Ioannidis JP, Evans SJ, Gotzsche PC et al. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004;141:781�8. doi:10.7326/0003-4819-141-10-200411160-00009[PubMed]
The most useful rule-of-thumb for headache and migraine treatment is: Have a program. See your doctor and produce a treatment strategy together. Your program will help you identify and handle migraines or your headaches early, sparing you some discomfort.
Tension Headache Treatments
When you get a pressure-type headache, it’s usually because of a change in neck, your mind, or encounter. Other tissues, nerves, blood vessels, and the muscles are experiencing distress. Treat the change, and you will reduce your headache.
It may build up unwanted stress, in case you have already been hunched over a laptop at work. Or perhaps a new medicine was started by you, or had minor neck injuries.
Take a minute curl up to stretch, or massage head your face, and neck. Consider a nap, a shower, or utilizing pack or ice pack on your own head or neck.
Tension Headache Medications
For tension headaches, you’ve numerous over-the-counter medicine alternatives. Naproxen ibuprofen, acetaminophen, and aspirin are successful. If you suspect your headache is vascular (associated to your own blood vessels), consider a pain-reliever that includes some caffeine.
Get in touch with your doctor for more tips if your headache does not react to to your own behavioral techniques and medications. In the event the headache becomes severe or lasts for more than 10 days, see your doctor. Your headache might be a signal of another condition.
Cluster Headache Treatments
Inhaling 100% oxygen right when a cluster headache starts can help lessen the pain considerably. Your doctor can help you get a portable oxygen unit to carry in a bag or briefcase.
A mainstay migraine medication, sumatriptan, is effective for cluster headaches. Learn to inject yourself right when you sense the first signs of your cluster headache. Other cluster headache medicines that are useful are dihydroergotamine, administered via an I-V, and octreotide sent as an injection.
Migraine Headache Prevention
Over the past 2 decades, health practitioners have realized effective treatments for decreasing the frequency of migraines. Avoid migraine triggers, take preventive medicine, alter your nourishment, and improve your rest.
One of numerous migraine triggers, several are foods, by avoiding so you can reduce your migraine risk:
Beans, legumes, and nuts
Fermented and pickled foods like pickles and olives
Dairy and cheese that is aged
Avocados
Onions
Cured or ag ed meats
Items containing brewer’s yeast
Chocolate, cocoa, and carob
Aspartame
Beverages
Caffeine
Other frequent migraine triggers include:
Stress
Weather changes
Poor diet
Hormonal changes
Nicotine
Physical activities that are intense
As you pay focus on what triggers your migraines, you are able to learn better what to avoid�??this is just a starting listing.
Your doctor will consider other medicines that prevent migraines. He/she might prescribe:
The blood-pressure drugs propranolol or timolol
Anti-depressants such as amitriptyline or fluoxetine
The seizure medication valproate
While these drugs came to market to handle other conditions, they are also efficient for migraine prevention.
Migraine Treatment
Migraine remedy is a race from the clock. You can take steps to reduce the intensity of the assault when you sense the warning signs of a migraine. That is the time to lie down, relax, and simply take your drugs.
Non-steroidal anti-inflammatories (NSAIDs), aspirin, and acetaminophen relieve some migraines. However, many migraine sufferers need stronger medicines for example sumatriptan or a different medication from your triptan family. In a few extreme circumstances, you may be treated by your physician with an opioid.
Treatments such as ice packs or cold compresses on your forehead rush instant reduction. Massaging your scalp and rubbing your temples may also help reduce the intensity of the migraine.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Cervicogenic Headache and Chiropractic
Neck pain associated with whiplash-associated disorders resulting from an automobile accident are reportedly the most prevalent cause for discomfort along the cervical spine. The sheer force of an impact from a rear-end car crash or other traffic incident can cause injuries or aggravate a previously existing condition. While neck pain is commonly the result of damage to the complex structures of the neck, cervicogenic headaches may also result due to neck issues. Chiropractic care can help carefully restore the alignment of the cervical spine to relieve headaches and neck pain.
El Paso, TX. Chiropractor Dr. Alex Jimenez looks at stretches for neck pain.
Your neck is one of the hardest working parts of your body.�It is serves us well as a source of strength and balance. When it�s out of whack, your neck can be a source of unending distress. �Let�s face it�today�s use of technology has our necks being put to use in ways it was never intended. �Did you know that looking down at your phone can sometimes exert as much pressure as the equivalent of a 40lb weight?
Unfortunately for the vast majority of people, neck pain will affect them at some point in their lives. Women are more prone to neck pain but men definitely have their fair share as well.
One Of The Reasons Our Necks Pay A Price… We Sit A Lot
Whether it is at home in front of the TV or electronics or at work in front of the computer, our necks get a work out! Distresses on the neck are felt in many ways, including but not limited to: low back pain, severe headache, migraines, or even facial aching and tenderness.
What are some of the gentle ways you can give your neck a break? Good question, we are glad you asked! Thankfully, stretching our neck muscles regularly is easy to do and it can help relieve and prevent neck pain.
El Paso, TX. Chiropractor Dr. Alex Jimenez investigates pain, the spine and its connection to internal organs.
Right after I had my first son, I suffered from headaches and some digestive issues. I had never had digestive issues before, but I passed it off as a side effect of giving birth to a living being. I also blamed the pressures of being in school and raising a small child.
My husband went to a chiropractor to treat some pain in his hands, and that is when I decided to try it as well. The chiropractor re-aligned my spine and, with weekly visits, I was feeling much better.
When my family and I moved to South Korea, I could not find a chiropractor. I did, however, find an excellent acupuncturist that had his office two blocks away from my front door. Instead of working on my spine, the acupuncturist worked on the muscles around my spine.
I feel the results of both were the same. I always felt much better when I took the time to take care of my spine and nervous system.
This is because all our organs receive messages from our brain via our spinal cord. The lungs know to breath in and out because of the messages they receive from the brain. The heart beats because of these messages as well. Every organ in our body is connected to the brain and blocking this connection�even a little�can cause serious health issues.
Some health problems are easily felt like numbness in the fingers or a headache. Some troubles are not so apparent like digestive issues or kidney problems. If the spine is out of order, the organs will feel it.
It Is Important To Take Care Of The Spine Every Day
If one takes a look at the image above, one can see how the nerves from the spinal cord connect to specific areas of the body. A chiropractor or acupuncturist will be able to spot spinal problems and fix them over time. This is what they are trained to do.
Here Are Some Tips To Take Care Of The Spine From Spine Health:
Sitting correctly or using an ergonomic chair while at work is a good way to take care of the spine.
Exercise abs and back daily to strengthen the muscles around the spine and keep it in place.
Take time to get a massage, see a chiropractor, or an acupuncturist. This will help the spine stay in the correct shape.
Wear shoes that support the feet and feel comfortable. Uncomfortable shoes, especially pumps, will injure the back and spine.
Sleep with the spine in mind. Choose a mattress and pillow that supports the spine and try to sleep in a natural position. Also, try sleeping on your arm to get a nice straight spine when lying on your side rather than using a pillow that can tilt your head up and kink your neck.
If one is suffering back pain, it is important to seek professional help. Spine problems, like a pinched nerve, if not taken care of, can become extremely severe. The spinal cord controls the body. In order to be in the best of health, the spine needs to be in good health.
Take care of�your spine and it will take care of you all the years of your life.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
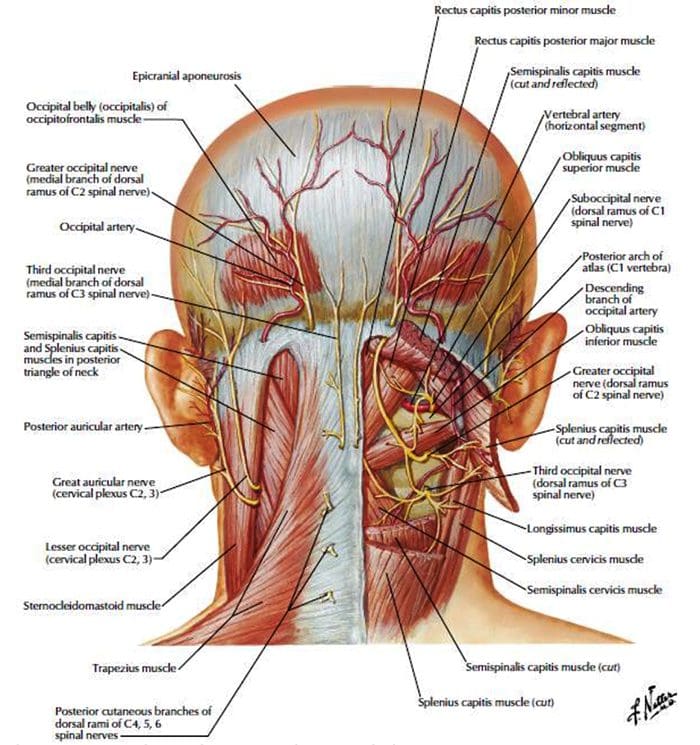 dailymedfact.com/neck-anatomy-the-suboccipital-triangle/
dailymedfact.com/neck-anatomy-the-suboccipital-triangle/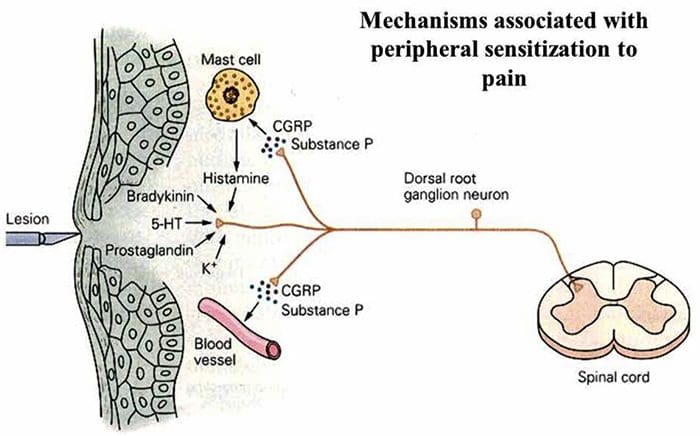 slideplayer.com/9003592/27/images/4/Mechanisms+associated+with+peripheral+sensitization+ to+pain.jpg
slideplayer.com/9003592/27/images/4/Mechanisms+associated+with+peripheral+sensitization+ to+pain.jpg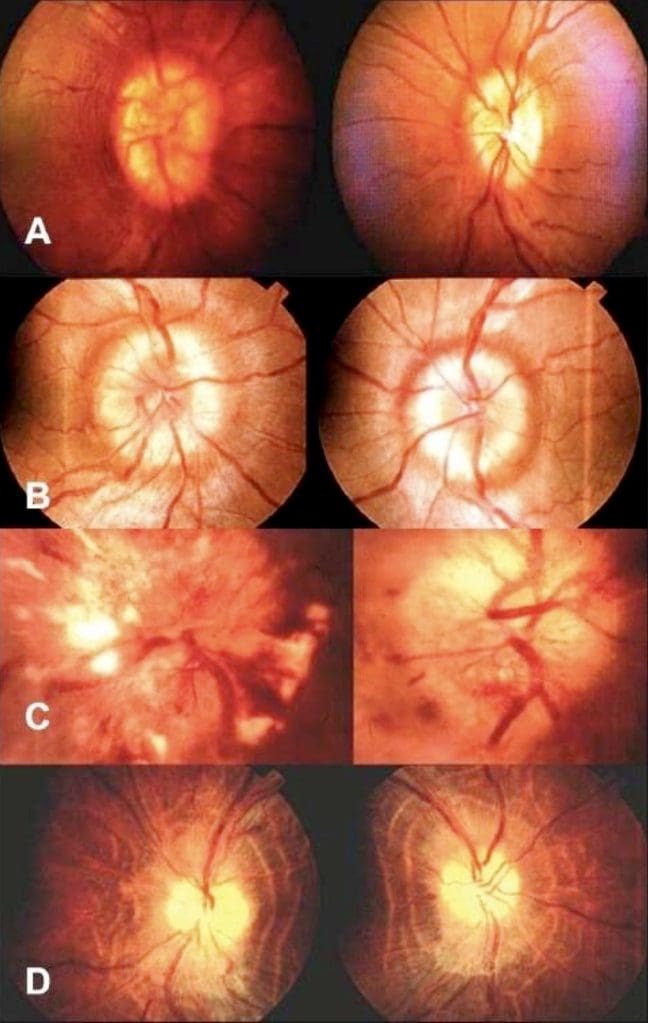
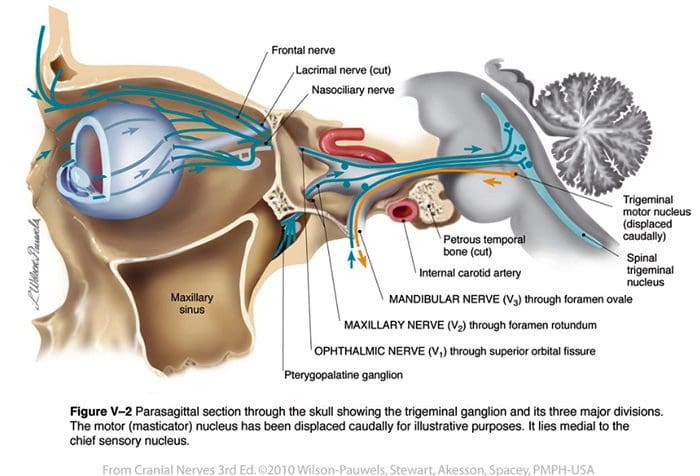









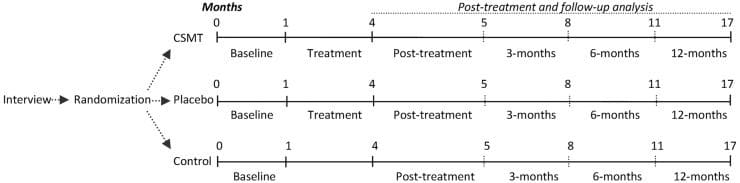


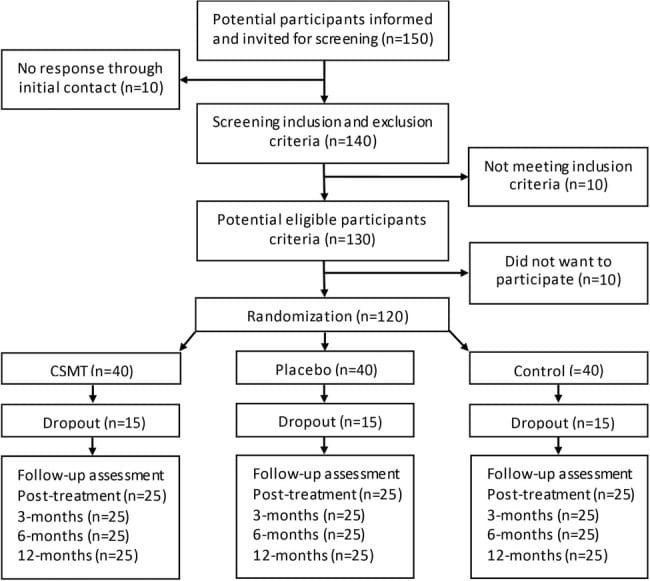


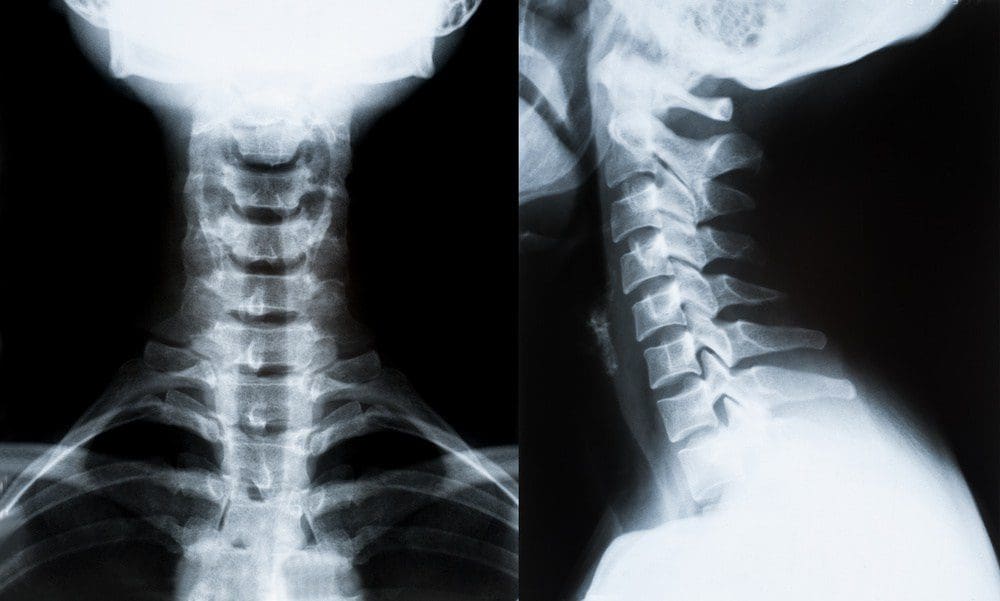






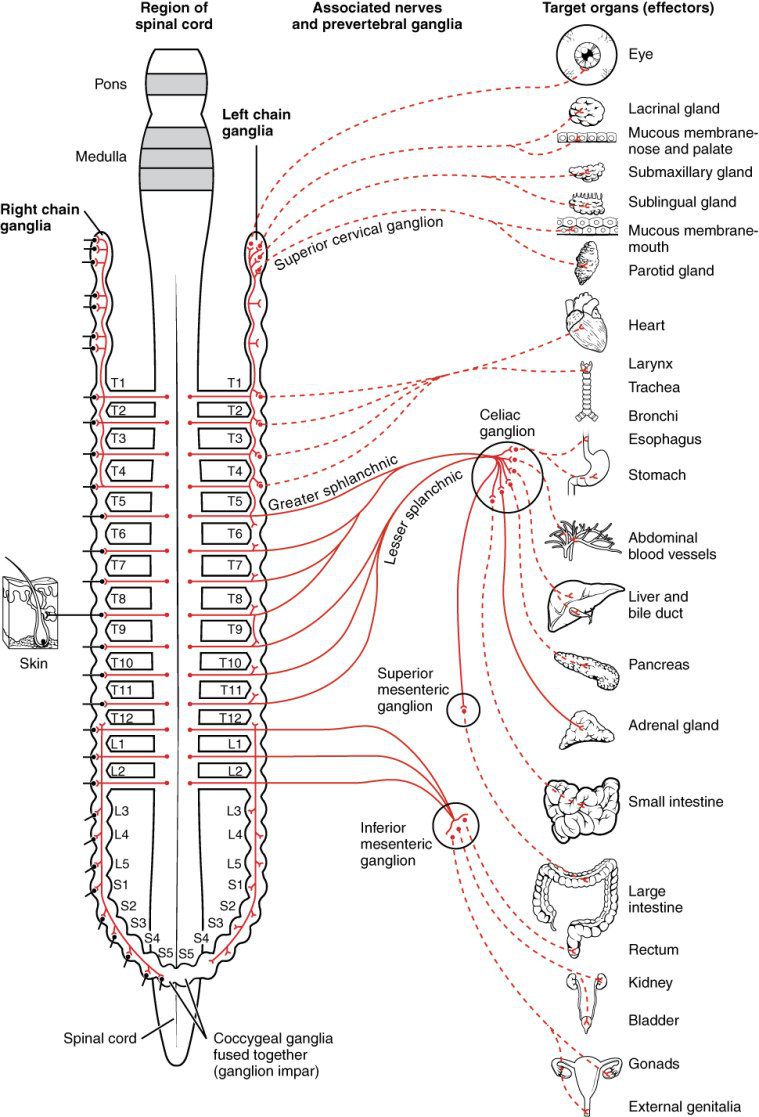







{kind=link}