Back Clinic Nerve Injury Team. Nerves are fragile and can be damaged by pressure, stretching, or cutting. Injury to a nerve can stop signals to and from the brain, causing muscles not to work properly and losing feeling in the injured area. The nervous system manages a great majority of the body’s functions, from regulating an individual’s breathing to controlling their muscles as well as sensing heat and cold. But, when trauma from an injury or an underlying condition causes nerve injury, an individual’s quality of life may be greatly affected. Dr. Alex Jimenez explains various concepts through his collection of archives revolving around the types of injuries and condition which can cause nerve complications as well as discuss the different form of treatments and solutions to ease nerve pain and restore the individual’s quality of life.
The information herein is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Individuals diagnosed with peripheral neuropathy, or with small fiber neuropathy, can understanding symptoms and causes help with potential treatments?
Small Fiber Neuropathy
Small fiber neuropathy is a specific classification of neuropathy, as there are different types, which are nerve injury, damage, disease, and/or dysfunction. Symptoms can result in pain, loss of sensation, and digestive and urinary symptoms. Most cases of neuropathy like peripheral neuropathy involve small and large fibers. Common causes include long-term diabetes, nutritional deficiencies, alcohol consumption, and chemotherapy.
Small fiber neuropathy is diagnosed after diagnostic testing showing it is clear that the small nerve fibers are involved.
The small nerve fibers detect sensation, temperature, and pain and help regulate involuntary functions.
Isolated small-fiber neuropathy is rare, but research is ongoing on the type of nerve damage and potential treatments. (Stephen A. Johnson, et al., 2021)
Small fiber neuropathy is not specifically dangerous but is a sign/symptom of an underlying cause/condition that is damaging the body’s nerves.
Pain – symptoms can range from mild or moderate discomfort to severe distress and can happen at any time.
Loss of sensation.
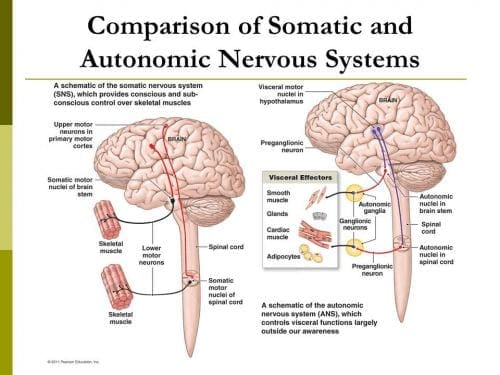
Because the small nerve fibers help with digestion, blood pressure, and bladder control – symptoms of autonomic dysfunction can vary and can include:
Constipation, diarrhea, incontinence, urinary retention – the inability to completely drain the bladder.
If there is progressing nerve damage, the intensity of the pain can decrease, but the loss of normal sensation and autonomic symptoms can worsen. (Josef Finsterer, Fulvio A. Scorza. 2022)
Hypersensitivity to touch and pain sensations can cause pain without a trigger.
The loss of sensation can make individuals unable to accurately detect sensations of touch, temperature, and pain in affected areas, which can lead to various types of injuries.
Although more research is needed, certain disorders that were not considered neuropathies may have small fiber neuropathy components involved.
A study suggested that neurogenic rosacea, a skin condition, could have some elements of small fiber neuropathy. (Min Li, et al., 2023)
These small nerve fibers are distributed throughout the body including the tops of the fingers and toes, trunk, and internal organs.
These fibers are usually located in the superficial areas of the body, such as close to the skin’s surface. (Mohammad A. Khoshnoodi, et al., 2016)
The small nerve fibers that get damaged are involved in transmitting pain and temperature sensations.
Most nerves have a special type of insulation called myelin that protects them and increases the speed of nerve impulses.
Small nerve fibers may have a thin sheath, making them more susceptible to injury and damage at earlier stages of conditions and diseases. (Heidrun H. Krämer, et al., 2023)
Individuals At Risk
Most types of peripheral neuropathy cause damage to the small and large peripheral nerve fibers. Because of this, most neuropathies are a mix of small-fiber and large-fiber neuropathy. Common risk factors for mixed fiber neuropathy include: (Stephen A. Johnson, et al., 2021)
Diabetes
Nutritional deficiencies
Overconsumption of alcohol
Autoimmune disorders
Medication toxicity
Isolated small-fiber neuropathy is rare, but there are conditions that are known to contribute to the cause and include: (Stephen A. Johnson, et al., 2021)
Sjogren Syndrome
This autoimmune disorder causes dry eyes and mouth, dental problems, and joint pain.
It can also cause nerve damage throughout the body.
Fabry Disease
This condition causes a buildup of certain fats/lipids in the body that can lead to neurological effects.
Amyloidosis
This is a rare disorder that causes a buildup of proteins in the body.
The proteins can damage tissues like the heart or nerves.
Lewy Body Disease
This is a neurological disorder that causes dementia and impaired movement and can lead to nerve damage.
Lupus
This is an autoimmune disease that affects joints, skin, and sometimes nerve tissue.
Viral Infection
These infections typically cause a cold or gastrointestinal/GI upsetness.
Less often they can cause other effects like small fiber neuropathy.
These conditions have been seen to cause isolated small-fiber neuropathy or begin as small-fiber neuropathy before progressing to the large nerve fibers. They can also begin as a mixed neuropathy, with small and large fibers.
Progression
Often the damage progresses at a relatively moderate rate, leading to added symptoms within months or years. The fiber nerves that are affected by the underlying condition usually progressively deteriorate, regardless of where they are located. (Mohammad A. Khoshnoodi, et al., 2016) Medications can help alleviate damage to the peripheral nerves. For individuals that are diagnosed in the early stage, it is possible to stop the progression, and potentially prevent involvement of the large fibers.
Treatments
Treatment toward preventing the progression requires controlling the underlying medical condition with treatment options depending on the cause. Treatments that can help prevent the progression include:
Blood sugar control for individuals with diabetes.
Immune suppression for control of autoimmune diseases.
Plasmapheresis – blood is taken and the plasma is treated and returned or exchanged for the treatment of autoimmune diseases.
Symptom Treatment
Individuals can get treatment for the symptoms that will not reverse or cure the condition but can help with temporary relief. Symptomatic treatment can include: (Josef Finsterer, Fulvio A. Scorza. 2022)
Pain management can include medications and/or topical analgesics.
Physical therapy – stretching, massage, decompression, and adjustments to keep the body relaxed and flexible.
Rehabilitation to help improve coordination, which can be impaired by loss of sensation.
Medications to relieve GI symptoms.
Wearing specialized clothes such as neuropathy socks to help with foot pain symptoms.
Treatment and medical management of neuropathies usually involve a neurologist. A neurologist may prescribe medication to help alleviate pain symptoms and provide medical interventions like immunotherapy if there is concern that an autoimmune process could be the cause. Additionally, treatment could include the care of a physical medicine and rehabilitation physician or a physical therapy team to provide stretches and exercises to help strengthen the body and maintain mobility and flexibility.
Peripheral Neuropathy Myths & Facts
References
Johnson, S. A., Shouman, K., Shelly, S., Sandroni, P., Berini, S. E., Dyck, P. J. B., Hoffman, E. M., Mandrekar, J., Niu, Z., Lamb, C. J., Low, P. A., Singer, W., Mauermann, M. L., Mills, J., Dubey, D., Staff, N. P., & Klein, C. J. (2021). Small Fiber Neuropathy Incidence, Prevalence, Longitudinal Impairments, and Disability. Neurology, 97(22), e2236–e2247. doi.org/10.1212/WNL.0000000000012894
Finsterer, J., & Scorza, F. A. (2022). Small fiber neuropathy. Acta neurologica Scandinavica, 145(5), 493–503. doi.org/10.1111/ane.13591
Krämer, H. H., Bücker, P., Jeibmann, A., Richter, H., Rosenbohm, A., Jeske, J., Baka, P., Geber, C., Wassenberg, M., Fangerau, T., Karst, U., Schänzer, A., & van Thriel, C. (2023). Gadolinium contrast agents: dermal deposits and potential effects on epidermal small nerve fibers. Journal of neurology, 270(8), 3981–3991. doi.org/10.1007/s00415-023-11740-z
Li, M., Tao, M., Zhang, Y., Pan, R., Gu, D., & Xu, Y. (2023). Neurogenic rosacea could be a small fiber neuropathy. Frontiers in pain research (Lausanne, Switzerland), 4, 1122134. doi.org/10.3389/fpain.2023.1122134
Khoshnoodi, M. A., Truelove, S., Burakgazi, A., Hoke, A., Mammen, A. L., & Polydefkis, M. (2016). Longitudinal Assessment of Small Fiber Neuropathy: Evidence of a Non-Length-Dependent Distal Axonopathy. JAMA neurology, 73(6), 684–690. doi.org/10.1001/jamaneurol.2016.0057
How does spinal decompression help reduce somatosensory pain associated with individuals dealing with back and leg pain?
Introduction
As we all know, the human body is a complex system that works together to perform various actions without feeling pain or discomfort. With muscles, organs, tissues, ligaments, bones, and nerve roots, each component has its job and interacts with other body parts. For instance, the spine collaborates with the central nervous system to instruct the muscles and organs to function correctly. Meanwhile, the nerve roots and muscles work together to provide mobility, stability, and flexibility to the upper and lower body extremities. However, as time passes, the body ages naturally, and this can lead to unwanted issues. Normal and traumatic factors can interfere with the neuron signals from the brain and cause somatosensory pain in the upper and lower extremities. This pain-like sensation can affect each body section, making the individual miserable. Luckily, there are ways to reduce somatosensory pain and provide relief to the body. Today’s article explores how somatosensory pain can impact the lower extremities, particularly the legs and back, and how non-surgical treatments like spinal decompression can alleviate somatosensory pain in the lower extremities. At the same time, we work hand-in-hand with certified medical providers who use our patient’s information to treat and mitigate somatosensory pain affecting the legs and back. We also inform them that non-surgical treatments like spinal decompression can help alleviate residual pain-like symptoms from the lower extremities. We encourage our patients to ask essential and important questions while seeking education from our associated medical providers about their pain. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
How Does Somatosensory Pain Affect The Legs & Back?
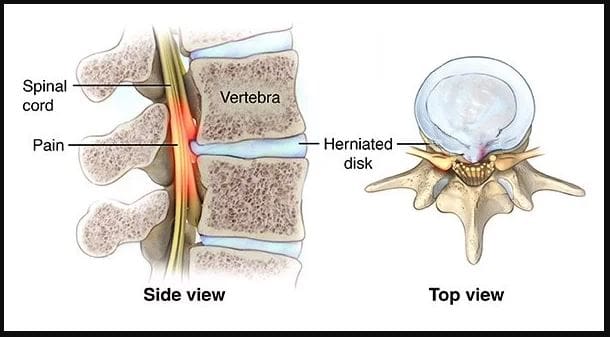
Are you experiencing numbness or tingling in your legs or back that disappears after a few minutes? Do you feel questionable pain in your lumbar spine after work? Or do you feel a warm sensation in the back of your legs that turns into sharp shooting pain? These issues may be related to the somatosensory system within the central nervous system, which provides voluntary reflexes to muscle groups. When normal movements or traumatic forces cause problems to the somatosensory system over time, it can lead to pain that affects the body’s extremities. (Finnerup, Kuner, & Jensen, 2021) This pain may be accompanied by burning, pricking, or squeezing sensations that affect the lumbar region. Many factors can be associated with somatosensory pain, which is part of the central nervous system and works with the spinal cord. When the spinal cord becomes compressed or aggravated due to injury or normal factors, it can lead to low back and leg pain. For example, a herniated disc in the lumbosacral area can cause nerve roots to send pain signals to the brain and cause abnormalities in the back and legs. (Aminoff & Goodin, 1988)
When people are dealing with back and leg pain from somatosensory pain, it can cause them to be miserable by reducing their quality of life and leading to a life of disability. (Rosenberger et al., 2020) At the same time, individuals dealing with somatosensory pain will also begin to feel inflammatory effects from the affected muscle area in the legs and back. Since inflammation is a body’s natural response when dealing with pain, the inflammatory cytokines can cause a cascading effect from the brain through the spinal cord, causing leg and back pain. (Matsuda, Huh, & Ji, 2019) To that point, somatosensory pain is associated with inflammation caused by normal or traumatic factors that can cause overlapping risk factors contributing to leg and back pain. Luckily, numerous treatments can reduce these overlapping risk factors caused by somatosensory pain and help restore the lower body extremities’ function.
Move Better, Live Better- Video
When the body is dealing with somatosensory pain, it can cause many individuals to think they are only dealing with one source of pain from one muscle area. Still, it can lead to multifactorial issues that affect different body locations. This is known as referred pain, where one body section deals with pain but is in a different area. Referred pain can also be combined with somato-visceral/visceral-somatic pain, where the affected muscle or organ affects one or the other, causing more pain-like issues. However, numerous treatments can reduce somatosensory pain from causing more leg and back problems. Non-surgical therapies like chiropractic care and spinal decompression can help mitigate the effects of somatosensory pain affecting the lower body extremities causing leg and back pain. These treatments allow the pain specialist to incorporate various therapeutic techniques to stretch the affected muscles and realign the spine to its original position. Many individuals can see an improvement in their mobility and daily activities as the pain-like symptoms associated with somatosensory pain are reduced. (Gose, Naguszewski, & Naguszewski, 1998) When individuals dealing with somatosensory pain start thinking about their health and wellness to ease the pain they are experiencing, they can look into non-surgical treatments as they are cost-effective, safe, and provide a positive outcome. Additionally, non-surgical treatments can be personalized to the individual’s pain and begin to see improvement after a few treatment sessions. (Saal & Saal, 1989) Check out the video above to learn more about how non-surgical treatments can be combined with other therapies to improve a person’s well-being.
Spinal Decompression Reduces Somatosenosory Pain
Now spinal decompression is a non-surgical treatment that can help reduce somatosensory pain affecting the legs and back. Since somatosensory pain correlates with the spinal cord, it can affect the lumbosacral spine and lead to back and leg pain. With spinal decompression, it utilizes gentle traction to gently pull the spine, which then can reduce the symptoms associated with somatosensory pain. Spinal decompression can help improve the somatosensory system by reducing pain and alleviating aggravated nerve root compression to relieve the legs and back. (Daniel, 2007)
Additionally, spinal decompression can be combined with other non-surgical treatments, like chiropractic, as it can help with reducing the effects of nerve entrapment and help restore the joint’s ROM (range of motion). (Kirkaldy-Willis & Cassidy, 1985) Spinal decompression can create a positive experience for many individuals dealing with leg and back pain associated with somatosensory pain while getting back their health and wellness.
References
Aminoff, M. J., & Goodin, D. S. (1988). Dermatomal somatosensory evoked potentials in lumbosacral root compression. J Neurol Neurosurg Psychiatry, 51(5), 740-742. doi.org/10.1136/jnnp.51.5.740-a
Daniel, D. M. (2007). Non-surgical spinal decompression therapy: does the scientific literature support efficacy claims made in the advertising media? Chiropr Osteopat, 15, 7. doi.org/10.1186/1746-1340-15-7
Finnerup, N. B., Kuner, R., & Jensen, T. S. (2021). Neuropathic Pain: From Mechanisms to Treatment. Physiol Rev, 101(1), 259-301. doi.org/10.1152/physrev.00045.2019
Gose, E. E., Naguszewski, W. K., & Naguszewski, R. K. (1998). Vertebral axial decompression therapy for pain associated with herniated or degenerated discs or facet syndrome: an outcome study. Neurol Res, 20(3), 186-190. doi.org/10.1080/01616412.1998.11740504
Kirkaldy-Willis, W. H., & Cassidy, J. D. (1985). Spinal manipulation in the treatment of low-back pain. Can Fam Physician, 31, 535-540. www.ncbi.nlm.nih.gov/pubmed/21274223
Matsuda, M., Huh, Y., & Ji, R. R. (2019). Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J Anesth, 33(1), 131-139. doi.org/10.1007/s00540-018-2579-4
Rosenberger, D. C., Blechschmidt, V., Timmerman, H., Wolff, A., & Treede, R. D. (2020). Challenges of neuropathic pain: focus on diabetic neuropathy. J Neural Transm (Vienna), 127(4), 589-624. doi.org/10.1007/s00702-020-02145-7
Saal, J. A., & Saal, J. S. (1989). Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study. Spine (Phila Pa 1976), 14(4), 431-437. doi.org/10.1097/00007632-198904000-00018
Are treatments more successful when patients know key terms that describe their back pain and associated conditions?
Nerve Pain Types
When individuals need to better understand their spine diagnosis, being able to distinguish between key terms can make a significant difference in understanding the development of a personalized treatment plan. Terms that describe back pain and various associated conditions can include:
Sciatica
Radiating and Referred pain
Radiculopathy
Radiculitis
Neuropathy
Neuritis
Causes of Back Pain
Back pain symptoms are most commonly caused by the continued practice of unhealthy/poor posture and overcompensated and weakened muscles. Even for individuals that exercise regularly, the movement choices that are made throughout the day can disrupt the way the muscles, tendons, ligaments, and fascia function to maintain proper body alignment.
Injuries to, and conditions of, the structures of the spinal column like the bones, discs, and nerves, are generally more serious than posture problems and soft tissue-related pain.
Depending on the diagnosis, structural problems can cause symptoms related to nerve compression, irritation, and/or inflammation. (Michigan Medicine, 2022)
Spine and Nervous System
The peripheral nerves extend out to the extremities with sensation and movement capabilities.
Nerve roots exit the spinal canal which is part of the peripheral nervous system.
The branching of nerves from the spinal cord and exit out of the foramina occurs at every level of the spine.
Terms
There are different medical terms when getting a spine diagnosis or going through the treatment process.
Radiculopathy
Radiculopathy is an umbrella term, describing any disease process that affects a spinal nerve root and is something that’s happening to the body.
When a healthcare provider informs you that your pain is due to radiculopathy, a number of more specific diagnoses, clinical signs, and symptoms may be included as part of the description.
Common causes of radiculopathy include herniated disc/s and spinal stenosis.
Less common causes can include a synovial cyst or tumor that presses on the nerve root. (Johns Hopkins Medicine, 2023)
Radiculopathy can occur in the neck, low back, or in the thoracic area.
Often, radiculopathy is brought on by some form of compression of the nerve root.
For example, extruded material from a herniated disc can land on a nerve root, causing pressure to build.
This can cause symptoms associated with radiculopathy, including numbness, weakness, pain, or electrical sensations. (Johns Hopkins Medicine, 2023)
Even though there’s a spinal nerve root on either side of the spinal column, injury, trauma, or issues stemming from degeneration affect the nerves in an asymmetric fashion. Degenerative changes, known as normal wear and tear, typically occur in this fashion. Using the previous herniated disc example, the material that leaks from the disc structure tends to travel in one direction. When this is the case, the symptoms tend to be experienced on the side where the nerve root makes contact with the disc material, but not the other side. (American Association of Neurological Surgeons, 2023)
Radiculitis
Radiculitis is a form of radiculopathy but it is about inflammation and not compression. (Johns Hopkins Medicine, 2023)
Radicu– refers to the spinal nerve root.
The suffix – itis refers to inflammation.
The word refers to a spinal nerve root that is inflamed and/or irritated rather than compressed.
In disc herniations, it is the gel substance that contains various chemicals that is inflammatory.
When the gel substance makes contact with nerve roots, an inflammatory response is triggered. (Rothman SM, Winkelstein BA 2007)
Radiating or Referred Pain
Radiating pain follows the path of one of the peripheral nerves that transmit sensory information like heat, cold, pins and needles, and pain.
Referred pain is experienced in a different area of the body that is away from the pain source which tends to be an organ. (Murray GM., 2009)
It can be brought on by myofascial trigger points or visceral activity.
An example of referred pain is symptoms in the jaw or arm when an individual is having a heart attack. (Murray GM., 2009)
Radicular
The terms radicular pain and radiculopathy tend to get confused.
Radicular pain is a symptom of radiculopathy.
Radicular pain radiates from the spinal nerve root to either part or all the way down the limb/extremity.
However, radicular pain does not represent the complete symptoms of radiculopathy.
Radiculopathy symptoms also include numbness, weakness, or electrical sensations like pins and needles, burning, or shock that travels down the extremity. (Johns Hopkins Medicine, 2023)
Neuropathy
Neuropathy is another umbrella term that refers to any dysfunction or disease that affects the nerves.
It’s usually classified according to the cause, like diabetic neuropathy, or the location.
Neuropathy can occur anywhere in the body – including the peripheral nerves, the autonomic nerves/organ nerves, or nerves that are located inside the skull and innervate the eyes, ears, nose, etc.
Peripheral nerves are the long, thin strands that supply sensation, feeling, and movement impulses to all areas of the body located outside the central nervous system.
Piriformis syndrome is where a tight buttock/piriformis muscle constricts the sciatic nerve, which runs underneath. (Cass SP. 2015)
Chiropractic
Chiropractic adjustments, non-surgical decompression, MET, and various massage therapies can relieve symptoms, release stuck or trapped nerves and restore function. Through the treatments, the chiropractor and therapists will explain what is happening and why they are using a specific technique. Knowing a little about how the neuromusculoskeletal system operates can help the healthcare provider and the patient in developing and adjusting effective treatment strategies.
Sciatica During Pregnancy
References
Michigan Medicine. Upper and Middle Back Pain.
American Academy of Neurological Surgeons. Anatomy of the Spine and Peripheral Nervous System.
Johns Hopkins Medicine. Health Conditions. Radiculopathy.
American Association of Neurological Surgeons. Herniated Disc.
American Academy of Orthopaedic Surgeons. OrthoInfo. Cervical Radiculopathy (Pinched Nerve).
Rothman, S. M., & Winkelstein, B. A. (2007). Chemical and mechanical nerve root insults induce differential behavioral sensitivity and glial activation that are enhanced in combination. Brain Research, 1181, 30–43. doi.org/10.1016/j.brainres.2007.08.064
American Academy of Orthopaedic Surgeons. OrthoInfo. Carpal Tunnel Syndrome.
Bostelmann, R., Zella, S., Steiger, H. J., & Petridis, A. K. (2016). Could Spinal Canal Compression be a Cause of Polyneuropathy? Clinics and practice, 6(1), 816. doi.org/10.4081/cp.2016.816
Cleveland Clinic. Mononeuropathy.
American Association of Neurological Surgeons. Glossary of Neurosurgical Terminology.
National Institutes of Health. U.S. National Library of Medicine. Medline Plus. Peripheral Nerve Disorders.
Cleveland Clinic. Spinal Stenosis.
Cass S. P. (2015). Piriformis syndrome: a cause of non-discogenic sciatica. Current sports medicine reports 14(1), 41–44. doi.org/10.1249/JSR.0000000000000110
The brachial plexus is a network of nerves that begin in the cervical/neck spinal cord and travel down the cervicoaxillary canal into the armpit. Forming in the area of the shoulder joint at the branch junction of the brachial plexus, the radial nerve extends down the arm, through the elbow joint, into the forearm, across the wrist, and tips of the fingers. The nerves are susceptible to injury that can cause abnormal function leading to unusual sensations and impaired muscle function.
Radial Nerve
One of the major nerves of the upper extremity.
There is one brachial plexus on each side of the body that carries the nerves to each arm.
The radial nerve has two major functions.
One is to provide sensations in the hands, forearms, arms, and fingers.
The other is to deliver messages to muscles about when to contract.
Motor Function
The radial nerve transmits signals to the muscles of the back of the arm and forearm on when to contract.
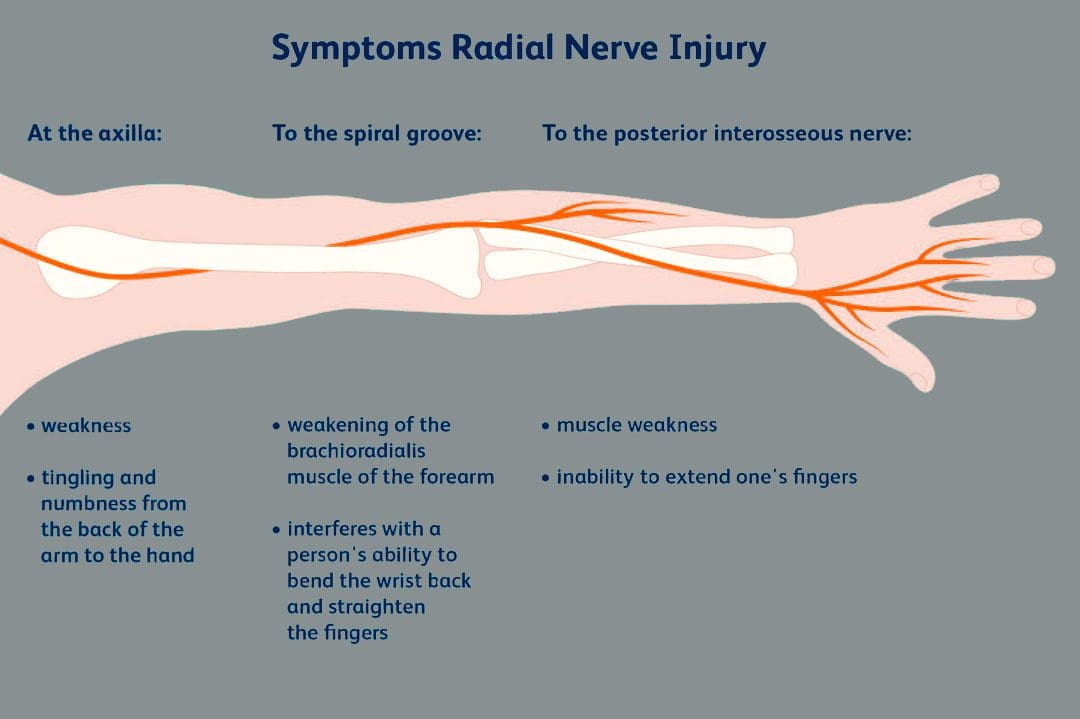
Individuals who have abnormal radial nerve function can experience weakness of the muscles and symptoms like wrist drop.
A wrist drop occurs when the back forearm muscles cannot support the wrist, causing the individual to hold the wrist in a flexed posture.
Abnormal radial nerve function can cause symptoms of numbness or tingling in the back of the hand.
Conditions
Associated conditions to the radial nerve include lacerations, contusions, fractures, and palsies.
Nerve Contusion
A contusion typically occurs through blunt force trauma that can crush and smash the nerve area.
This causes abnormal or no function.
A nerve contusion can occur from a personal, work, or sports injury or other conditions that generate intense pressure on the nerve/s.
Nerve Lacerations
A laceration occurs when there is a penetrating injury that cuts and/or severs the nerve.
This injury can occur from stab wounds or sliced by broken glass, metal, etc.
Fractures
Broken bones of the upper extremity can lead to extended damage to the nerves near the damaged bone.
The most common type of fracture associated with radial nerve malfunction is fractures to the humerus bone.
The nerve wraps tightly around the humerus and can be injured with a fracture.
Most fracture-related radial nerve injuries heal on their own and do not require surgery.
However, the way the injury heals can be the difference between normal function and chronic pain.
Crutch Palsy
Crutch palsy is pressure on the radial nerve in the armpit resulting from using crutches incorrectly.
To use crutches properly, the individual needs to support their body weight through the hands.
However, many tend to place pressure around the armpit at the top of the crutch, causing irritation to the nerve in that area.
Padding the top of crutches and using the proper form can prevent the condition.
Saturday Night Palsy
Saturday night palsy is the abnormal function of the radial nerve after sleeping in a position that causes direct pressure against the nerve.
This often occurs when an individual falls asleep with their arm draped over an armrest on a chair.
The name comes from when individuals are intoxicated and fall asleep in a location other than the bed and in awkward positions.
Treatment
Nerve injuries often cause symptoms at different locations other than where the nerve damage is, complicating diagnosis. Determining the specific location of nerve damage is the first step in developing an appropriate treatment plan. Once the location has been identified, steps can be taken to prevent worsening damage to the nerve.
The objective is to relieve the pressure from the irritation or compression.
Massage to relax the area and increase blood circulation.
Decompression to physically restore alignment.
Adjustments to restore body balance.
Exercises and stretches to maintain treatment, strengthen the muscles, and prevent injuries.
In cases where there is structural damage, surgery may be necessary to remove pressure or repair damage.
Avoid Surgery
References
Ansari FH, Juergens AL. Saturday Night Palsy. [Updated 2023 Apr 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK557520/
Barton, N J. “Radial nerve lesions.” The Hand vol. 5,3 (1973): 200-8. doi:10.1016/0072-968x(73)90029-6
Daly, Michael, and Chris Langhammer. “Radial Nerve Injury in Humeral Shaft Fracture.” The Orthopedic Clinics of North America vol. 53,2 (2022): 145-154. doi:10.1016/j.ocl.2022.01.001
DeCastro A, Keefe P. Wrist Drop. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK532993/
Eaton, C J, and G D Lister. “Radial nerve compression.” Hand Clinics vol. 8,2 (1992): 345-57.
Glover NM, Murphy PB. Anatomy, Shoulder and Upper Limb, Radial Nerve. [Updated 2022 Aug 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK534840/
Ljungquist, Karin L et al. “Radial nerve injuries.” The Journal of hand surgery vol. 40,1 (2015): 166-72. doi:10.1016/j.jhsa.2014.05.010
A nerve becomes pinched/compressed when added pressure is placed on it by surrounding structures that can include muscles, bones, ligaments, tendons, or a combination. This injures and damages the nerve causing function problems and symptoms and sensations in that area or other parts of the body that are supplied by that nerve. Medical practitioners refer to this as nerve compression or entrapment. Although compressed nerves are more commonly associated with the neck, arms, hands, elbows, and lower back, any nerve in the body can experience irritation, spasms, inflammation, and compression. The causes and treatment of a compressed nerve in the knee.
Compressed Nerve In The Knee
There’s only one nerve that goes through the knee that has an increased risk of getting compressed. It’s a branch of the sciatic nerve called the peroneal nerve. The nerve goes around the outside of the knee before traveling down the outside of the lower leg. At the bottom of the knee, it lies between the bone and skin, making it vulnerable to irritation or compression by anything that can put pressure on the outside of the knee.
Causes
Traumatic injuries over time can lead to pressure on the nerve from inside the knee. Common causes of a compressed nerve in the knee include:
Frequently Crossing Legs
Compression by the opposite knee, while the legs are crossed is the most common cause.
Knee Brace
A too-tight or strong brace can compress the leg and nerve.
Thigh-High Compression Stockings
Designed to maintain pressure on the legs, if too tight these stockings can compress the nerve.
Squatting Posture For Long Periods
This position places pressure on the side of the knee.
Fractures
A fracture of the large lower leg bone/tibia or sometimes the small bone/fibula near the knee can entrap the nerve.
Lower Leg Cast
The portion of the cast around the knee can be tight and compress the nerve.
Tell the doctor if a cast or brace feels tight or is causing numbness or pain in the leg.
Knee-High Boots
The top of a boot can land right below the knee and be too tight pinching the nerve.
Knee Ligament Injury
The nerve can become compressed due to bleeding or inflammation from an injured ligament.
Knee Surgery Complications
This is rare, but the nerve can inadvertently get pinched during knee replacement surgery or an arthroscopic procedure.
Prolonged Bed Rest
When lying down the legs tend to rotate outward and the knees flex.
In this position, the mattress can place pressure on the nerve.
Tumors or Cysts
Tumors or cysts can develop right on top or next to a nerve irritating and compressing the area.
Abdominal or Gynecologic Surgery
The equipment used to keep the legs rotated outward and the knees flexed for gynecologic and abdominal surgeries can compress the nerve.
Symptoms
The peroneal nerve supplies sensation and movement to the outside of the lower leg and the top of the foot. When compressed, it becomes inflamed, which causes the symptoms of a compressed nerve. Usually, only the lining/myelin sheath around the nerve is what gets injured. However, when the nerve gets damaged, the symptoms are similar but more severe. Common symptoms include:
Weakness that limits the ability to lift the foot toward the leg aka dorsiflexion.
This causes dragging the foot when walking.
The ability to turn the foot outward and extend the big toe is also affected.
Symptoms can be felt on the outside of the lower leg and on the top of the foot and include:
Tingling or pins and needles sensations.
Numbness.
Loss of sensation.
Pain.
Burning.
For individuals that have had a pinched nerve for two or more weeks, the muscles supplied by the nerve can begin to waste away or atrophy.
Symptoms can be intermittent or continuous depending on the cause.
The other common cause is a pinched nerve in the lumbar/lower spine.
When this is the cause, sensations, and pain will present in the lower back or the back and outside of the thigh.
Diagnosis
A doctor will look at medical history and perform an examination to make a diagnosis, determine the cause, and lay out a personalized treatment plan. The nerve in the knee can be felt as it travels around the top of the tibia, so a doctor may tap on it. If there is shooting pain down the leg, a pinched nerve may be present. Tests a doctor may order can include:
Knee X-ray
Shows any bone fractures or abnormal masses.
Knee MRI
Can confirm the diagnosis
Shows masses within the nerve.
Shows details of fractures or other problems in the bones.
Electromyogram – EMG
Tests electrical activity in the muscles.
Nerve Conduction Test
Tests the signal speed of the nerve.
Treatment
Treatment is aimed at reducing pain and improving mobility.
Over-the-Counter Pain Medication
OTC medication can reduce inflammation and improve symptoms short term.
Ice and Heat
Applying either heat or ice for 15 to 20 minutes at a time can provide relief from the symptoms.
An ice pack can make symptoms worse if it adds more pressure on the nerve.
Chiropractic and Physical Therapy
Chiropractic and physical therapy can release the compressed nerve, realign the structures, strengthen the muscles, and provide gait training.
Orthotic Boot
If walking gait is affected because the foot cannot bend, an orthotic boot can help.
This is a support that maintains the foot in a neutral position to walk normally.
Corticosteroid Injection
A corticosteroid injection can reduce inflammation and relieve pressure on the nerve.
Surgery
The nerve can suffer permanent damage if it has been pinched for a long time.
If that happens, surgery cannot repair the damage.
A doctor can perform surgery to correct a fracture, tumor, or other invasive problem causing a compressed nerve.
If conservative treatment doesn’t work, a peroneal nerve decompression procedure can be done to remove the pressure.
If surgery is needed, symptoms can disappear immediately, but it takes around four months to recover and rehabilitate.
Injury Rehabilitation
References
Krych, Aaron J et al. “Is peroneal nerve injury associated with worse function after knee dislocation?.” Clinical orthopedics and related research vol. 472,9 (2014): 2630-6. doi:10.1007/s11999-014-3542-9
Lezak B, Massel DH, Varacallo M. Peroneal Nerve Injury. [Updated 2022 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK549859/
Soltani Mohammadi, Sussan, et al. “Comparing the squatting position and traditional sitting position for ease of spinal needle placement: a randomized clinical trial.” Anesthesiology and pain medicine vol. 4,2 e13969. 5 Apr. 2014, doi:10.5812/aapm.13969
Stanitski, C L. “Rehabilitation following knee injury.” Clinics in sports medicine vol. 4,3 (1985): 495-511.
Xu, Lin, et al. Zhongguo gu Shang = China Journal of Orthopedics and Traumatology vol. 33,11 (2020): 1071-5. doi:10.12200/j.issn.1003-0034.2020.11.017
Yacub, Jennifer N et al. “Nerve injury in patients after hip and knee arthroplasties and knee arthroscopy.” American Journal of physical medicine & Rehabilitation vol. 88,8 (2009): 635-41; quiz 642-4, 691. doi:10.1097/PHM.0b013e3181ae0c9d
The neck is an extremely flexible part of the upper body that allows the head to move without causing pain or discomfort. It is part of the musculoskeletal system‘s cervical spinal region, which supports the spinal column and is surrounded by various muscles, tissues, and ligaments that protect the spinal cord. However, poor posture, spending too much time hunched over a computer, or looking down at our cellphones can cause neck muscles to become overstretched, leading to compression of the cervical spinal discs. This can cause the cervical discs to bulge or herniate, aggravating the spinal cord and causing neck pain and other associated conditions. This post will discuss how cervical disc compression affects neck pain and how decompression surgery and spinal decompression can help alleviate this condition. We work with certified medical providers who use our patients’ valuable information to treat individuals dealing with cervical disc compression affecting their necks and causes mobility issues. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
What Is Cervical Disc Compression?
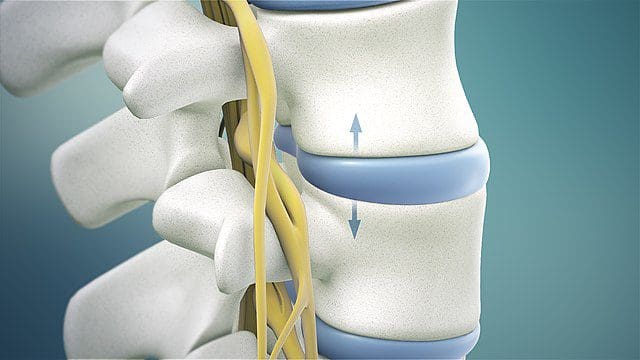
Have you been experiencing neck pain or muscle aches in your shoulders? Do you feel numbness or tingling running down your arms and fingers? These symptoms may be signs of cervical disc compression. The cervical spinal discs act as shock absorbers for the spine, preventing unwanted pressure and mobility issues. Research studies revealed that age-related degenerative properties like dehydration could cause herniated and compressed cervical discs, leading to posterior disc protrusion into the spinal cord. Trauma can also cause extreme hyperflexion or hyperextension of the posterior neck muscles, resulting in various neck symptoms. Additional research studies stated cervical disc displacement could cause compression or impingement on spinal nerve roots, leading to inflammation and neck pain.
How Is It Associated With Neck Pain?
When the spinal cord and nerve roots in the cervical region are affected by cervical disc compression, the pain can be dull or sharp, depending on how it affects many individuals. According to research studies, many people are unaware that repetitive normal factors or traumatic forces can cause a challenge in determining the origin of the pain from symptomatic or asymptomatic disc compression. Additional research studies mentioned that cervical disc compression could cause upper and lower extremities abnormalities, such as loss of deep tendon reflexes in the arms and legs, loss of motor function in the hands and feet, muscle weakness, headaches, and gait imbalances. However, various treatments can alleviate the pain-like symptoms associated with cervical disc compression and help the body’s natural healing process.
From Inflammation To Healing-Video
Are you experiencing inflammation and pain in your neck? Do you notice a tingling or numb sensation in your hands or feet? Or do you feel stiffness in your shoulders or neck? These symptoms can be caused by compressed cervical discs, which many people are unaware of. The compression of cervical discs is a common source of neck pain and can even cause referred pain in the upper and lower extremities. Repetitive motions to the neck can cause the posterior neck muscles to overstretch and lead to pain. Normal or traumatic factors can also lead to neck pain associated with cervical disc compression, resulting in disc herniation. Fortunately, non-surgical therapies like chiropractic care and spinal decompression can help alleviate the symptoms of pain, discomfort, and inflammation caused by cervical disc compression. Check out the video above for more information on these treatments.
Posterior Cervical Disc Decompression Surgery
If you experience cervical compression on your neck, it can lead to persistent neck pain and discomfort if left untreated. Many people opt for posterior cervical disc decompression surgery to alleviate the effects of disc herniation. According to “The Ultimate Spinal Decompression” by Dr. Perry Bard, D.C., and Dr. Eric Kaplan, D.C., FIAMA, cervical disc herniation can sometimes affect the back of the neck and cause persistent pain. In such cases, decompression surgery is often performed. During the procedure, a small incision is made at the back of the neck, and a portion of the damaged disc is removed to ease the irritated nerve. This brings relief to the individual suffering from neck pain.
Non-Surgical Decompression For Compressed Cervical Disc
If you’re not interested in surgery for cervical disc compression, consider non-surgical spinal decompression instead. Studies have shown that spinal decompression is a safe, non-invasive treatment involving gentle cervical spine traction to reposition the herniated disc. This treatment can also help rehydrate the spinal disc by bringing in nutrients and oxygenated blood to promote natural healing. Additionally, spinal decompression can alleviate any remaining symptoms of neck pain.
Conclusion
The neck is a highly flexible area that enables smooth head movement without discomfort or pain. However, it is also a part of the musculoskeletal cervical region that can be prone to injuries. Compression of the disc due to normal or traumatic factors can result in herniation, causing pain if left untreated. Fortunately, several treatments are available to alleviate neck pain caused by cervical compression and make the neck mobile again.
When temperatures are elevated in summer, heat-induced and severe headaches like migraines are common during the hot months. However, a migraine caused by heat is not the same as a headache caused by heat, as the two have different symptoms. What they have in common is that they’re both triggered by the way hot weather affects the body. Understanding the causes and the warning signs of a heat headache can help prevent and treat potentially dangerous heat-related conditions. Injury Medical Chiropractic and Functional Medicine Clinic use various techniques and therapies customized to the individual to relieve pain and improve function.
Heat-Induced Headaches
Headaches and migraines are common, affecting 20 percent of women and nearly 10 percent of men. An increase in frequency can be caused by
Dehydration.
Environmental factors.
Heat exhaustion.
Heat stroke.
A heat-induced headache can feel like a dull pulsing ache around the temples or in the back of the head. Depending on the cause, a heat-induced headache may escalate to a more intensely felt internal pain.
Causes
A heat-induced headache may not be caused by the hot weather but by how the body responds to heat. Weather-related triggers of headaches and migraine include:
Hormonal fluctuations are common migraine triggers that can also cause headaches.
Dehydration – can trigger both headaches and migraine.
When exposed to higher temperatures, the body needs more water to compensate for the lost water as it uses and sweats it out. Prolonged exposure to high temperatures puts the body at risk for heat exhaustion, one of the stages of heat stroke, with headaches as a symptom of heat exhaustion. Any time the body is exposed to high temperatures or spends a long time outside in the hot sun, and a headache occurs afterward, a heat stroke is possible.
Heat Headache Symptoms
Symptoms of a heat-induced headache can vary according to the situation. If the headache is triggered by heat exhaustion, the body will have heat exhaustion symptoms and head pain. Heat exhaustion symptoms include:
Dizziness.
Muscle cramps or tightness.
Nausea.
Fainting.
An extreme thirst that does not go away.
If the headache or migraine is related to heat exposure but not connected to heat exhaustion, the symptoms may include the following:
A throbbing, dull sensation in the head.
Dehydration.
Fatigue.
Sensitivity to light.
Relief
Individuals can be proactive about prevention.
If possible, limit time outside, protect the eyes with sunglasses, and wear a hat with a brim when staying outdoors.
Exercise indoors in an air-conditioned environment if able.
Increase water consumption as temperatures rise, and utilize healthy sports drinks to replenish electrolytes.
Craniocervical mobilization involves gentle chiropractic pressure on the neck to adjust the joints.
Spinal manipulation involves applying more force and pressure at certain points along the spine.
Neuromuscular massage includes kneading joints and muscles and relieves pain by releasing pressure from compressed nerves.
Myofascial release massage is aimed at the tissues that connect and support muscles and focuses on trigger points in the back and neck or head to relax muscles and improve blood circulation.
Trigger point therapies target tense areas to help relax muscles while improving blood flow and relieving stress.
Traction therapy.
Decompression therapy.
Exercises designed specifically to reduce pain.
From Inflammation to Healing
References
Bryans, Roland, et al. “Evidence-based guidelines for the chiropractic treatment of adults with headache.” Journal of Manipulative and physiological therapeutics vol. 34,5 (2011): 274-89. doi:10.1016/j.jmpt.2011.04.008
Demont, Anthony, et al. “Efficacy of physiotherapy interventions for the management of adults with cervicogenic headache: A systematic review and meta-analyses.” PM & R: the journal of Injury, Function, and Rehabilitation vol. 15,5 (2023): 613-628. doi:10.1002/pmrj.12856
Di Lorenzo, C et al. “Heat stress disorders and headache: a case of new daily persistent headache secondary to heat stroke.” BMJ case reports vol. 2009 (2009): bcr08.2008.0700. doi:10.1136/bcr.08.2008.0700
Fernández-de-Las-Peñas, César, and María L Cuadrado. “Physical therapy for headaches.” Cephalalgia: an international journal of Headache vol. 36,12 (2016): 1134-1142. doi:10.1177/0333102415596445
Swanson JW. (2018). Migraines: Are they triggered by weather changes? mayoclinic.org/diseases-conditions/migraine-headache/expert-answers/migraine-headache/faq-20058505
Victoria Espí-López, Gemma, et al. “Effectiveness of Physical Therapy in Patients with Tension-type Headache: Literature Review.” Journal of the Japanese Physical Therapy Association = Rigaku ryoho vol. 17,1 (2014): 31-38. doi:10.1298/jjpta.Vol17_005
Whalen, John, et al. “A Short Review of the Treatment of Headaches Using Osteopathic Manipulative Treatment.” Current pain and headache reports vol. 22,12 82. 5 Oct. 2018, doi:10.1007/s11916-018-0736-y
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine