Back Clinic Chiropractic Spine Care Team. The spine is designed with three natural curves; the neck curvature or cervical spine, the upper back curvature or thoracic spine, and the lower back curvature or lumbar spine, all of which come together to form a slight shape when viewed from the side. The spine is an essential structure as it helps support the upright posture of humans, it provides the body with the flexibility to move and it plays the crucial role of protecting the spinal cord. Spinal health is important in order to ensure the body is functioning to its fullest capacity. Dr. Alex Jimenez strongly indicates across his collection of articles on spine care, how to properly support a healthy spine. For more information, please feel free to contact us at (915) 850-0900 or text to call Dr. Jimenez personally at (915) 540-8444.
“Various problems with the sacrum make up or contribute to a significant portion of lower back problems. Can understanding the anatomy and function help prevent and treat back injuries?”
The Sacrum
The sacrum is a bone shaped like an upside-down triangle located at the base of the spine that helps support the upper body when sitting or standing and provides pelvic girdle flexibility during childbirth. It comprises five vertebrae that fuse during adulthood and connect to the pelvis. This bone takes and endures all of the body’s pressure and stress from everyday activities and movements.
Formation
Humans are born with four to six sacral vertebrae. However, fusion does not take place in all sacral vertebrae simultaneously:
Fusion starts with the S1 and S2.
As the individual gets older, the overall shape of the sacrum begins to solidify, and the vertebrae fuse into a single structure.
The process usually starts in the mid-teens and finishes in the early to mid-twenties.
It is believed to start earlier in females than males.
The sacrum in a female is wider and shorter and has a more curved top or the pelvic inlet.
The male sacrum is longer, narrower, and flatter.
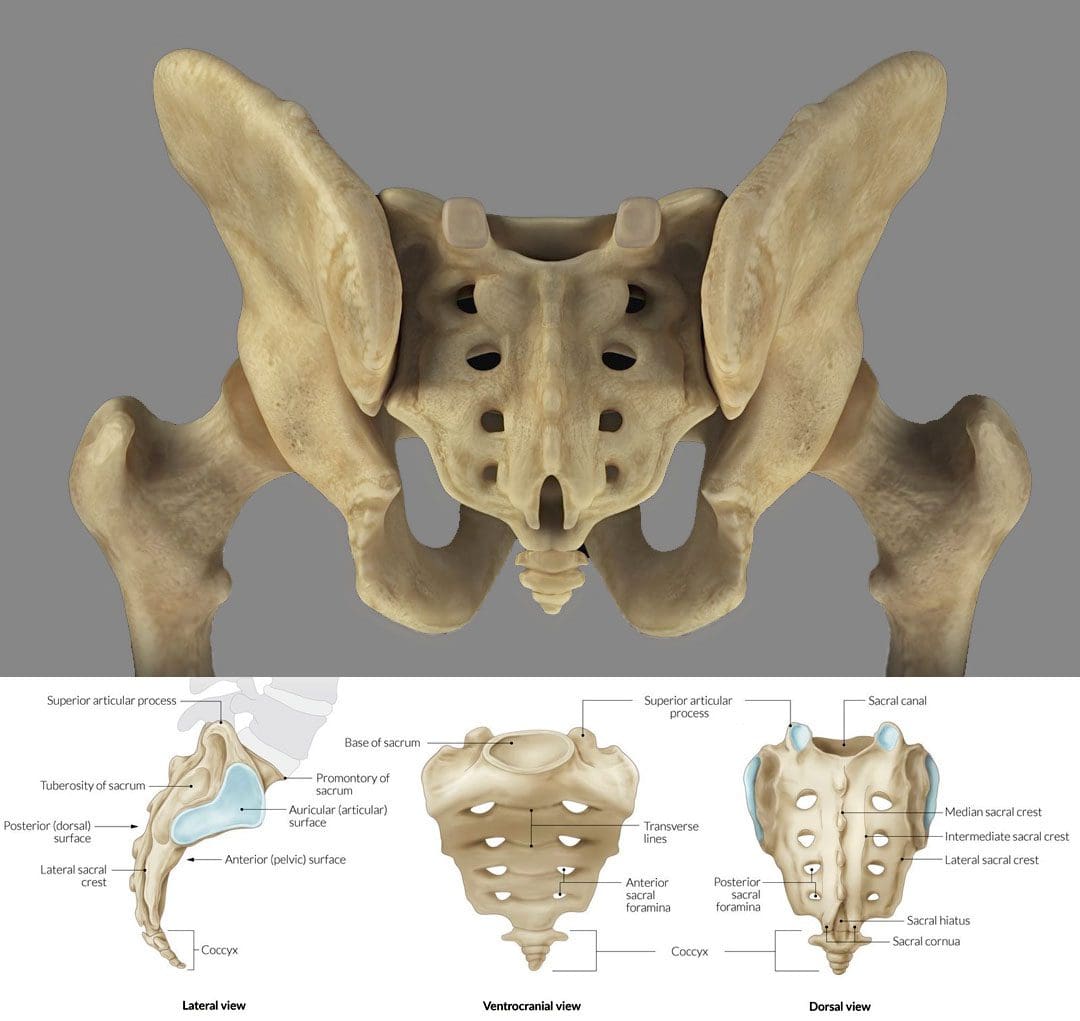
Structure
The sacrum is an irregular bone that makes up the back/posterior third of the pelvic girdle. There is a ridge across the front/anterior portion of the S1 vertebra known as the sacral promontory. Small holes/foramen on both sides of the sacrum are left over after the vertebrae fuse together. Depending on the number of vertebrae, there can be three to five foramen on each side, though there are usually four. (E. Nastoulis, et al., 2019)
Each anterior foramen is typically wider than the posterior or dorsal/backside foramen.
Each sacral foramina/plural of foramen provides a channel for the sacral nerves and blood vessels.
Small ridges develop between each of the fused vertebrae, known as transverse ridges or lines.
The top of the sacrum is called the base and is connected to the largest and lowest of the lumbar vertebrae – L5.
The bottom is connected to the tailbone/coccyx, known as the apex.
The sacral canal is hollow, runs from the base to the apex, and serves as a channel at the end of the spinal cord.
The sides of the sacrum connect to the right and left hip/iliac bones. The attachment point is the auricular surface.
Right behind the auricular surface is the sacral tuberosity, which serves as an attachment area for the ligaments that hold the pelvic girdle together.
Location
The sacrum is at the level of the lower back, just above the intergluteal cleft or where the buttocks split. The cleft starts at around the level of the tailbone or coccyx. The sacrum is curved forward and ends at the coccyx, with the curvature being more pronounced in females than males. It connects to the L5 lumbar vertebra by way of the lumbosacral joint. The disc between these two vertebrae is a common source of low back pain.
On either side of the lumbosacral joint are wing-like structures known as the sacral ala, which connect to the iliac bones and form the top of the sacroiliac joint.
These wings provide stability and strength for walking and standing.
Anatomical Variations
The most common anatomical variation applies to the number of vertebrae. The most common is five, but anomalies have been documented, including individuals with four or six sacral vertebrae. (E. Nastoulis, et al., 2019)
Other variations involve the sacrum’s surface and curvature, where the curvature differs widely between individuals.
In some cases, the first and second vertebrae do not fuse and remain separately articulated.
Failure of the canal to completely close during formation is a condition known as spina bifida.
Function
Studies on the sacrum are ongoing, but some proven functions include:
It serves as an anchor point for the spinal column to attach to the pelvis.
It provides stability for the body’s core.
It acts as a platform for the spinal column to rest on when sitting.
It facilitates childbirth, providing pelvic girdle flexibility.
It supports upper body weight when sitting or standing.
It provides extra stability for walking, balance, and mobility.
Conditions
The sacrum can be a main source or focal point for lower back pain. It is estimated that 28% of men and 31.6% of women aged 18 years or older have experienced low back pain in the past three months. (Centers for Disease Control and Prevention. 2020) Conditions that can cause sacrum pain symptoms include.
Sacroiliitis
This is a common condition of sacroiliac/SI joint inflammation.
A doctor only makes the diagnosis when all other possible causes of pain have been ruled out, known as a diagnosis of exclusion.
About half of all chordomas form in the sacrum, but the tumors can also develop elsewhere in the vertebral column or at the base of the skull. (National Library of Medicine. 2015)
Spina Bifida
Individuals can be born with conditions that affect the sacrum.
Spina bifida is a congenital condition that can arise from the malformation of the sacral canal.
Unlocking the Secrets of Inflammation
References
Gruss, L. T., & Schmitt, D. (2015). The evolution of the human pelvis: changing adaptations to bipedalism, obstetrics and thermoregulation. Philosophical transactions of the Royal Society of London. Series B, Biological sciences, 370(1663), 20140063. doi.org/10.1098/rstb.2014.0063
Nastoulis, E., Karakasi, M. V., Pavlidis, P., Thomaidis, V., & Fiska, A. (2019). Anatomy and clinical significance of sacral variations: a systematic review. Folia morphologica, 78(4), 651–667. doi.org/10.5603/FM.a2019.0040
Barros, G., McGrath, L., & Gelfenbeyn, M. (2019). Sacroiliac Joint Dysfunction in Patients With Low Back Pain. Federal practitioner : for the health care professionals of the VA, DoD, and PHS, 36(8), 370–375.
Can various therapeutic options provide relief for individuals with upper crossed syndrome to restore muscle strength?
Introduction
Many individuals often suffer neck and shoulder pain from poor posture, improper heavy lifting, musculoskeletal conditions, auto accidents, whiplash, etc. The surrounding muscles that connect the neck and shoulders help protect the cervical and thoracic region of the spine and can succumb to injuries that can cause pain-like symptoms causing discomfort to the individual. Neck, shoulder, and back pain are the three most common issues many individuals have experienced. These musculoskeletal disorders can also correlate with pre-existing conditions; many people will feel pain and discomfort while trying to find the relief they seek. One of the most common issues people often experience is upper crossed syndrome, which can be associated with neck and shoulder pain. Today’s article explains what upper cross syndrome is and how it affects the neck and shoulders while also diving into how different therapeutic options like spinal decompression and chiropractic care can reduce the effects of upper cross syndrome. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to mitigate upper-crossed syndrome in the neck and shoulders. We also inform our patients that there are many therapeutic options, like chiropractic care and spinal decompression, to minimize muscle pain in the neck and shoulders. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with upper-crossed syndrome. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer
What Is Upper Crossed Syndrome?
Have you been dealing with muscle pain in your shoulders or neck after being on the computer for a while? Do you feel stiffness in your shoulders that rotating them causes temporary relief? Or does it hurt when you turn your head from side to side? Many of these pain-like scenarios are often associated with upper-cross syndrome. Many people don’t often realize that upper crossed syndrome is a musculoskeletal condition that affects the neck, shoulder, and chest muscles and causes them to be weak and tight due to poor posture. The upper crossed syndrome can cause referred pain to the upper extremities, leading to cervicogenic headaches, limited range of motion, trigger points in the muscles, and muscle imbalance. (Moore, 2004) When many people are dealing with upper crossed syndrome due to poor posture, it can lead to many issues in the neck and shoulders.
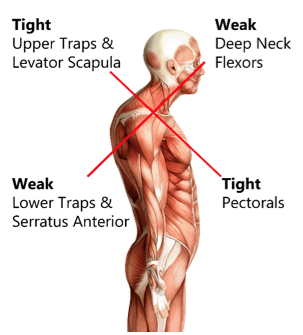
How Does It Affect The Neck & Shoulders?
Now, why does upper crossed syndrome affect the neck and shoulders? Many people unintentionally hunched over when looking at their phones, being on the computer, or relaxing at home. This causes specific muscles in the neck and shoulder region, like the serratus and lower trapezius muscles, to become weak while the pectoral and neck muscles are tight. (Chu & Butler, 2021) This, in turn, causes the shoulders to be more rounded and hunched, causing the neck and head to crane forward. When people are dealing with upper crossed syndrome, many would often complain about pain-like symptoms like:
Headaches
Neck Strain
Muscle tightness
Upper back pain
Restricted range of motion
Numbness/Tingling sensations in the arms
The upper crossed syndrome can also occur gradually over time and cause nerve compression to the upper extremities. When the upper neck and shoulder muscles start to affect the surrounding nerve roots, which then leads to nerve dysfunction in the sensory and motor skills when a person picks up an object. (Lee & Lim, 2019) However, many individuals dealing with upper-crossed syndrome can seek treatment to relieve muscle pain in their neck and shoulders.
An Overview Of Upper Crossed Syndrome- Video
Since upper cross syndrome is a musculoskeletal condition that affects the neck and shoulders, it can result in muscle imbalance and pain in the individual. Many people, especially in the working field, develop this syndrome by being hunched over for an extended period. (Mujawar & Sagar, 2019) This causes the head to be more forward, the neck posture to be curved and hunched, and the shoulders to be rounded. The video above explains upper-crossing syndrome, its causes, and how it is treated.
Numerous treatments can help restore muscle strength and reduce muscle pain in the neck and shoulders. Treatments like spinal decompression can help reduce upper crossed syndrome by slowly using gentle traction to the cervical spine region and gently stretching the neck muscles to provide relief. Spinal decompression is one of the non-surgical treatments that many individuals with headaches associated with upper crossed syndrome can find the comfort they seek through pain reduction and improve their quality of life. (Eskilsson et al., 2021) At the same time, spinal decompression can be part of a personalized treatment plan that many individuals can add to their daily routine to prevent the pain from returning. (Saunders, 1983)
Chiropractic Care Restoring Muscle Strength
Just like spinal decompression, chiropractic care is a non-surgical treatment that can be combined with various stretching techniques to restore the neck’s range of motion and reduce pain associated with upper-crossed syndrome. (Mahmood et al., 2021) Chiropractic care incorporates manual and mechanical techniques like MET (muscle energy techniques) and spinal manipulation to realign the spine out of subluxation. When chiropractors integrate MET to manage upper crossed syndrome, many individuals find that their pain has decreased, their cervical range of motion is improved, and their neck disability is reduced. (Gillani et al., 2020) When many individuals start thinking about their health and wellness, they can make small changes to improve their posture and be more mindful of their bodies to reduce the chances of upper-cross syndrome returning.
References
Chu, E. C., & Butler, K. R. (2021). Resolution of Gastroesophageal Reflux Disease Following Correction for Upper Cross Syndrome-A Case Study and Brief Review. Clin Pract, 11(2), 322-326. doi.org/10.3390/clinpract11020045
Eskilsson, A., Ageberg, E., Ericson, H., Marklund, N., & Anderberg, L. (2021). Decompression of the greater occipital nerve improves outcome in patients with chronic headache and neck pain – a retrospective cohort study. Acta Neurochir (Wien), 163(9), 2425-2433. doi.org/10.1007/s00701-021-04913-0
Gillani, S. N., Ain, Q., Rehman, S. U., & Masood, T. (2020). Effects of eccentric muscle energy technique versus static stretching exercises in the management of cervical dysfunction in upper cross syndrome: a randomized control trial. J Pak Med Assoc, 70(3), 394-398. doi.org/10.5455/JPMA.300417
Lee, E. Y., & Lim, A. Y. T. (2019). Nerve Compression in the Upper Limb. Clin Plast Surg, 46(3), 285-293. doi.org/10.1016/j.cps.2019.03.001
Mahmood, T., Afzal, W., Ahmad, U., Arif, M. A., & Ahmad, A. (2021). Comparative effectiveness of routine physical therapy with and without instrument assisted soft tissue mobilization in patients with neck pain due to upper crossed syndrome. J Pak Med Assoc, 71(10), 2304-2308. doi.org/10.47391/JPMA.03-415
Moore, M. K. (2004). Upper crossed syndrome and its relationship to cervicogenic headache. J Manipulative Physiol Ther, 27(6), 414-420. doi.org/10.1016/j.jmpt.2004.05.007
Mujawar, J. C., & Sagar, J. H. (2019). Prevalence of Upper Cross Syndrome in Laundry Workers. Indian J Occup Environ Med, 23(1), 54-56. doi.org/10.4103/ijoem.IJOEM_169_18
Saunders, H. D. (1983). Use of spinal traction in the treatment of neck and back conditions. Clin Orthop Relat Res(179), 31-38. www.ncbi.nlm.nih.gov/pubmed/6617030
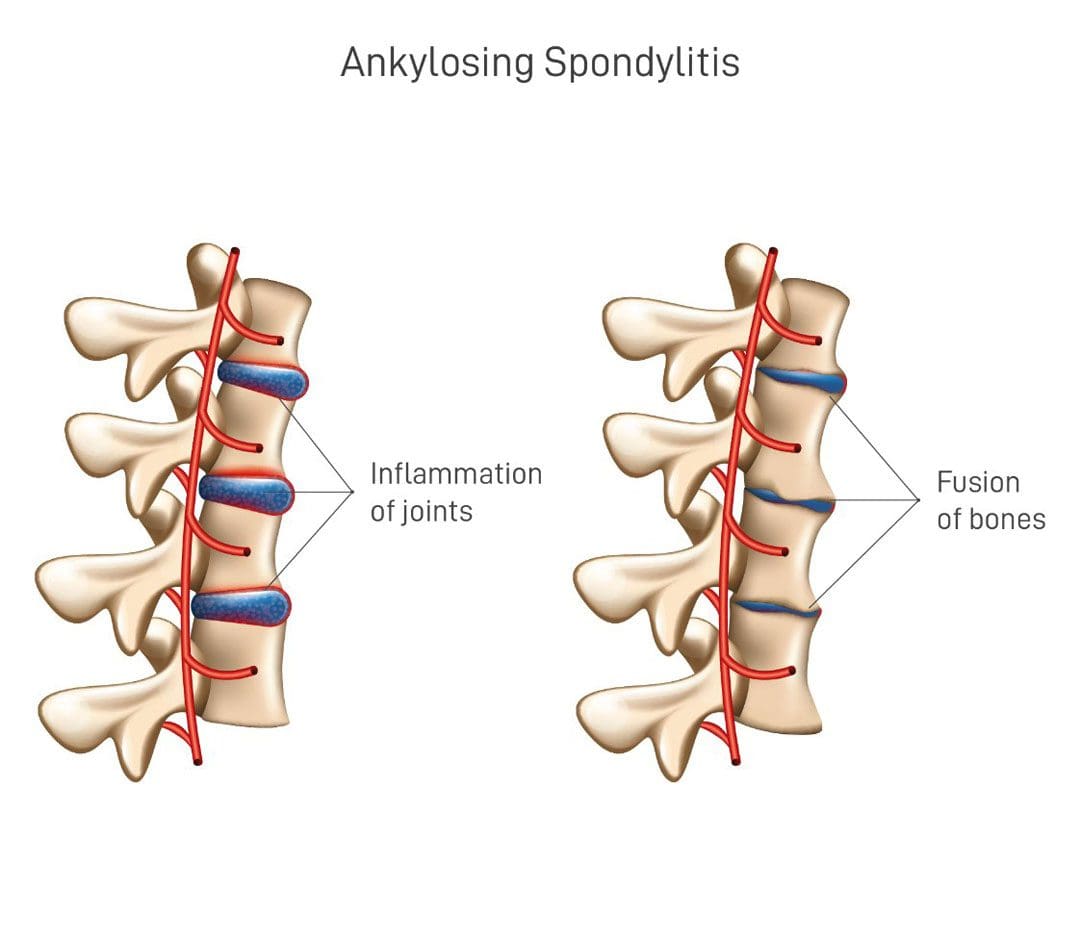
Ankylosing spondylitis is an inflammatory arthritis that causes changes in posture that occur over time. Can exercise and maintaining spinal alignment help improve posture problems?
Ankylosing Spondylitis Posture Improvement
Ankylosing spondylitis/AS is an autoimmune arthritis that primarily affects the spine. It can also spread to other joints of the body and affect the internal organs. Back pain problems are a common side effect of the condition and depending on the severity of damage to the spine, it can have a serious impact on posture.
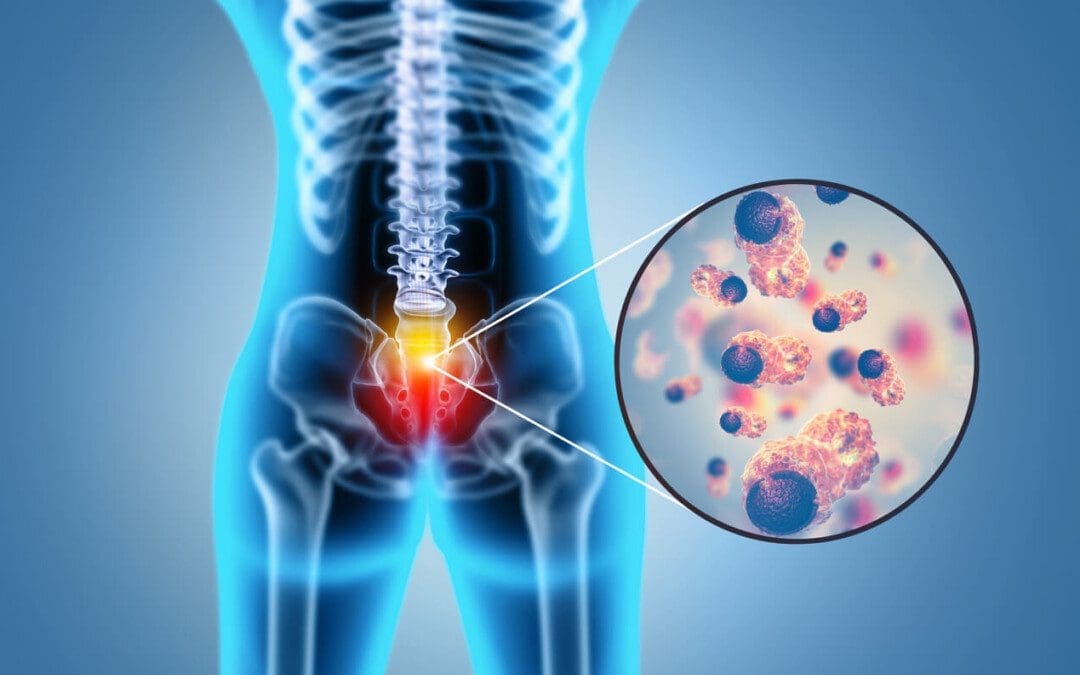
Affects Posture
The condition usually first affects the sacroiliac joints at the bottom of the spine where they attach to the pelvis. As the condition progresses it works its way to the upper spine. The spine consists of 26 vertebrae/bones stacked on top of each other.
Line up the ears, shoulders, hips, knees, and ankles in a straight line.
Squeeze the shoulder blades together and down toward the back pockets.
Relax the arms at the sides.
Look straight ahead.
Tuck the chin back slightly.
Sitting
The natural curves of the spine need support for proper posture when sitting. Try these tips when at a desk or at a table:
Position the height of the chair so the hips and knees are bent at 90-degree angles.
Place the feet flat on the floor or use a footstool based on chair height.
Place a lumbar support pillow or rolled-up towel behind the lower back.
Position the screen monitor at eye level to keep the upper back straight.
Keep the keyboard and mouse close to the body to prevent overreaching which can increase the rounding of the shoulders and upper back.
Lying Down
Ankylosing spondylitis can make lying down uncomfortable. To support the spine while lying down try to:
Sleep on a semi-firm mattress or type like memory foam to conform to the body.
Place a pillow between the knees to maintain a straight spine when lying on the side.
Use a specialized pillow to prevent placing the upper back in a rounded position.
Posture Exercises
For individuals with ankylosing spondylitis stretching and strengthening exercises can help improve body posture. Individuals are recommended to talk to their healthcare provider before beginning an exercise program.
Chin Tucks
Sit up straight.
Squeeze the shoulder blades together.
Rest the arms at your sides.
Look straight ahead, pull the chin back and in until the stretch is felt along the muscles of the neck.
Hold for three to five seconds and relax.
Repeat 10 times.
Corner Stretch
Stand facing a corner.
Raise the arms to shoulder height.
Place one forearm flat against each wall.
Stagger the feet.
Slowly shift weight over the front leg and lean in toward the corner.
Stop once the stretch is felt across the chest.
Hold for 10 to 20 seconds and relax.
Repeat three times.
Scapular Squeezes
Sit up straight with arms resting at the sides.
Squeeze the shoulder blades together like they are holding an object between them.
Hold for three seconds and relax.
Repeat 10 times.
Maintaining spinal alignment will help decrease back pain that occurs with AS.
Targeted exercises can help stretch tight muscles and strengthen the muscles responsible for maintaining spinal alignment.
Maintaining healthy posture when sitting, standing, and sleeping can help prevent deformities in the spine.
Regular physical activity can help combat stiffness and help maintain overall strength.
For an individualized exercise program, see a physical therapist or chiropractor on incorporating posture exercises to help prevent complications from developing.
Arthritis
References
National Institute of Arthritis and Musculoskeletal and Skin Diseases. Ankylosing spondylitis.
De Nunzio, A. M., Iervolino, S., Zincarelli, C., Di Gioia, L., Rengo, G., Multari, V., Peluso, R., Di Minno, M. N., & Pappone, N. (2015). Ankylosing spondylitis and posture control: the role of visual input. BioMed research international, 2015, 948674. doi.org/10.1155/2015/948674
How can spinal decompression reduce pain while restoring spinal flexibility in many individuals with lumbar degenerative disorders?
Introduction
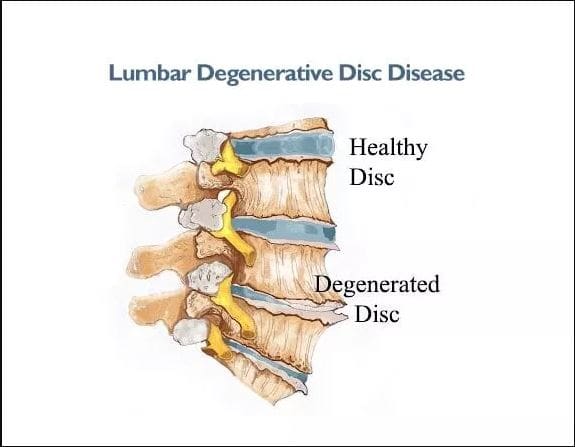
As we naturally age, so do our spines and spinal discs, as the natural fluids and nutrients stop hydrating the discs and cause them to degenerate. When disc degeneration starts to affect the spine, it can cause pain-like symptoms in the lumbar regions, which then develop into lower back pain or other musculoskeletal disorders that affect the lower extremities. When disc degeneration starts to affect the lumbar region, many individuals will notice that they are not as flexible as when they were younger. The physical signs of straining their muscles from improper lifting, falling, or carrying heavy objects can cause muscle strain and pain. When this happens, many individuals will treat the pain with home remedies, which can provide temporary relief but can aggravate it more when people make repetitive motions to their lumbar spine, which can result in injuries. Fortunately, non-surgical treatments that can help slow down the process of disc degeneration while rehydrating the spinal disc. Today’s article looks at why disc degeneration affects lumbar flexibility and how treatments like spinal decompression reduce disc degeneration while restoring lumbar flexibility. Coincidentally, we communicate with certified medical providers who incorporate our patients’ information to provide various treatment plans to reduce the disc degeneration process and provide pain relief. We also inform them that there are non-surgical options to reduce the pain-like symptoms associated with disc degeneration and help restore lumbar flexibility. We encourage our patients to ask amazing educational questions to our associated medical providers about their symptoms correlating with body pain in a safe and positive environment. Dr. Alex Jimenez, D.C., incorporates this information as an academic service. Disclaimer
How Does DDD Affect Lumbar Flexibility?
Have you been experiencing stiffness in your back when you wake up in the morning? Do you feel muscle aches and pains when bending down and picking up heavy objects? Or do you feel radiating pain in your legs and back? When many individuals are in excruciating pain, many don’t often realize that their lower back pain could also be associated with their spinal disc degenerating. Since the spinal disc and the body can degenerate naturally, it can lead to the development of musculoskeletal disorders. DDD, or degenerative disc disease, is a common disabling condition that can greatly impact the musculoskeletal system and is the main cause of individuals missing out on their daily activities. (Cao et al., 2022) When normal or traumatic factors begin to cause repetitive motions to the spine, it can cause the spinal disc to be compressed and, over time, degenerate. This, in turn, causes the spine to be less flexible and becomes a socio-economic challenge.
When disc degeneration starts to cause spinal inflexibility, it can lead to the development of low back pain. Since low back pain is a common health concern, it can affect many individuals worldwide, as disc degeneration is a common factor. (Samanta et al., 2023) Since disc degeneration is a multi-factorial disorder, the musculoskeletal and organ systems are also affected as it can cause referred pain to different body locations. Luckily, many individuals can find the treatment they are looking for, as many seek relief from the many pain issues that disc degeneration has caused.
Lumbar Spine Injuries In Athletes- Video
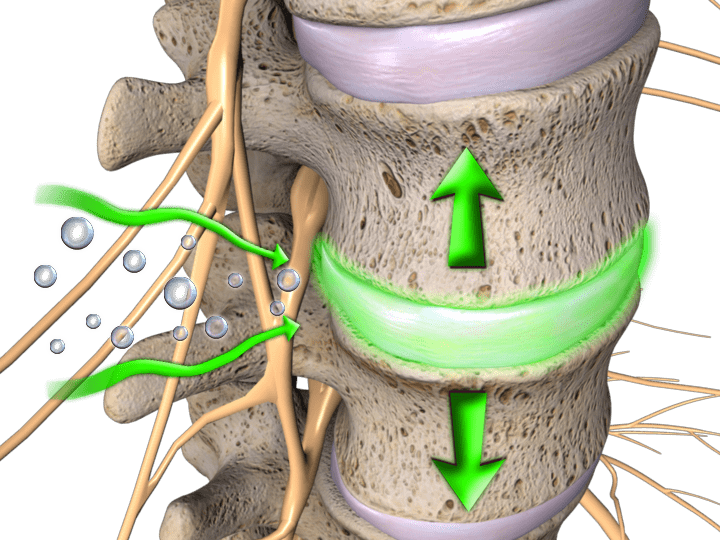
Since disc degeneration is a multi-factorial cause of disability, it can become a primary source of back pain. When normal factors contribute to back pain, it likely correlates with disc degeneration and can cause cellular, structural, compositional, and mechanical changes throughout the spine. (Ashinsky et al., 2021) However, many individuals seeking treatment can look into non-surgical therapies as they are cost-effective and safe on the spine. Non-surgical treatments are safe and gentle on the spine as they can be customizable to the person’s pain and combined with other treatment forms. One of the non-surgical treatments is spinal decompression, which uses gentle traction on the spine to rehydrate the spinal disc from degeneration and help kick-start the body’s natural healing process. The video above shows how disc degeneration is correlated with disc herniation and how these treatments can reduce its pain-like effects on the spine.
Spinal Decompression Reducing DDD
When many individuals are going in for treatment for disc degeneration, many will often try spinal decompression as it is affordable. Many healthcare professionals will assess the individual by creating a personalized plan before entering the traction machine. Many individuals will get a CT scan to assess the changes caused by DDD. (Dullerud & Nakstad, 1994) This determines how severe the disc space is. The traction machine for spinal decompression determines the optimal treatment duration, frequency, and mode of administrating traction to the spine to reduce DDD. (Pellecchia, 1994) Additionally, the efficiency of traction from spinal decompression can help many people with low back and provide relief. (Beurskens et al., 1995)
References
Ashinsky, B., Smith, H. E., Mauck, R. L., & Gullbrand, S. E. (2021). Intervertebral disc degeneration and regeneration: a motion segment perspective. Eur Cell Mater, 41, 370-380. doi.org/10.22203/eCM.v041a24
Beurskens, A. J., de Vet, H. C., Koke, A. J., Lindeman, E., Regtop, W., van der Heijden, G. J., & Knipschild, P. G. (1995). Efficacy of traction for non-specific low back pain: a randomised clinical trial. Lancet, 346(8990), 1596-1600. doi.org/10.1016/s0140-6736(95)91930-9
Cao, G., Yang, S., Cao, J., Tan, Z., Wu, L., Dong, F., Ding, W., & Zhang, F. (2022). The Role of Oxidative Stress in Intervertebral Disc Degeneration. Oxid Med Cell Longev, 2022, 2166817. doi.org/10.1155/2022/2166817
Dullerud, R., & Nakstad, P. H. (1994). CT changes after conservative treatment for lumbar disk herniation. Acta Radiol, 35(5), 415-419. www.ncbi.nlm.nih.gov/pubmed/8086244
Pellecchia, G. L. (1994). Lumbar traction: a review of the literature. J Orthop Sports Phys Ther, 20(5), 262-267. doi.org/10.2519/jospt.1994.20.5.262
Samanta, A., Lufkin, T., & Kraus, P. (2023). Intervertebral disc degeneration-Current therapeutic options and challenges. Front Public Health, 11, 1156749. doi.org/10.3389/fpubh.2023.1156749
Can healthcare professionals help individuals with spinal pain by incorporating non-surgical spinal decompression to restore mobility?
Introduction
Many individuals don’t realize that putting unwanted pressure on their spines can lead to chronic pain within their spinal discs that is affecting their spinal mobility. This usually happens with demanding jobs requiring individuals to carry heavy objects, step wrong, or be physically inactive, which causes the surrounding back muscles to be overstretched and leads to referred pain that affects the upper and lower body portions. This can cause individuals to go to their primary doctors to get treated for back pain. This leads to them missing out on their busy work schedules and paying a high price to get treated. Back pain correlating with spinal issues can be a huge problem and make them feel miserable. Fortunately, numerous clinical options are cost-effective and personalized to many individuals dealing with spinal pain that is causing them to find the relief they deserve. Today’s article focuses on why spinal pain affects many people and how spinal decompression can help reduce spinal pain and restore spinal mobility. Coincidentally, we communicate with certified medical providers who incorporate our patients’ information to provide various treatment plans to reduce spinal pain affecting their backs. We also inform them that there are non-surgical options to reduce the pain-like symptoms associated with spinal issues in the body. We encourage our patients to ask amazing educational questions to our associated medical providers about their symptoms correlating with body pain in a safe and positive environment. Dr. Alex Jimenez, D.C., incorporates this information as an academic service. Disclaimer
Why Spinal Pain Is Affecting Many People?
Have you often experienced pain from your back muscles that seem to ache after bending down constantly to pick up objects? Do you or your loved ones feel muscle stiffness in the back and experience numbness in your upper or lower body portions? Or are you experiencing temporary relief after stretching your back muscles, only for the pain to return? Many individuals with back pain never realize that their pain is within their spinal column. Since the spine is an S-curve shape with three different regions in the body, the spinal discs within each spinal segment can become compressed and become misaligned over time. This causes degenerative changes within the spine and can cause the three different spinal regions to develop pain-like issues in the body. When several environmental factors start to be the causes of degeneration of the spinal discs, it can affect the spinal structure. It can become a strong influence affecting their function, predisposing the disc to injuries. (Choi, 2009) At the same time, this can cause a significant impact when getting treated due to its high cost and can start normal age-related changes that cause pathophysiological issues to the vertebral body. (Gallucci et al., 2005)
When many individuals are dealing with spinal pain associated with herniated discs, it can not only cause discomfort but also mimic other musculoskeletal disorders that can cause radiating pain to different locations in the body. (Deyo et al., 1990) This, in turn, causes individuals to suffer constantly and research various treatments to reduce the pain they are experiencing. When spinal pain affects most individuals, many will seek cost-effective therapies to ease the pain they are experiencing and to be mindful of the daily habits they adopt over time and correct them.
Spinal Decompression In-Depth- Video
Do you often feel constant muscle aches and pains in your body that are your general areas of complaint? Do you feel your muscles pull uncomfortably after lifting or carrying a heavy object? Or do you feel constant stress in your neck, shoulders, or back? When many individuals are dealing with general pain, they often assume that it is just back pain when it could be a spinal issue that can be the root cause of the pain they are experiencing. When this happens, many individuals opt for non-surgical treatments due to its cost-effectiveness and how it can be personalized depending on the severity of the pain. One of the non-surgical treatments is spinal decompression/traction therapy. The video above gives an in-depth look at how spinal decompression can help reduce spinal pain associated with low back pain. Spinal pain can increase with age and be provoked by extreme lumbar extension, so incorporating spinal decompression can help reduce pain in the upper and lower extremities. (Katz et al., 2022)
How Spinal Decompression Can Reduce Spinal Pain
When individuals develop spinal issues, spinal decompression can help restore the spine to its original position and help the body naturally heal itself. When something is out of place within the spine, it is important to naturally restore it to its proper place to allow the affected muscles to heal. (Cyriax, 1950) Spinal decompression uses gentle traction to pull the spinal joints to let the spinal disc back in its original position and help increase fluid intake back in the spine. When people start incorporating spinal decompression into their health and wellness routine, they can reduce their spinal pain after a few consecutive treatments.
Spinal Decompression Restoring Spinal Mobility
Spinal decompression can also be incorporated with other non-surgical treatments to restore spinal mobility. When pain specialists utilize spinal decompression within their practices, they can help treat various musculoskeletal conditions, including spinal disorders, to allow the individual to regain spinal mobility. (Pettman, 2007) At the same time, pain specialists can use mechanical and manual manipulation to reduce the pain the individual feels. When spinal decompression starts to use gentle traction on the spine, it can help minimize radical pain correlated with nerve entrapment, create negative pressure within the spinal sections, and relieve musculoskeletal disorders causing pain. (Daniel, 2007) When people start thinking more about their health and wellness to reduce their pain, spinal decompression can be the answer through a personalized plan and can help many individuals find the relief they deserve.
References
Choi, Y. S. (2009). Pathophysiology of degenerative disc disease. Asian Spine Journal, 3(1), 39-44. doi.org/10.4184/asj.2009.3.1.39
Daniel, D. M. (2007). Non-surgical spinal decompression therapy: does the scientific literature support efficacy claims made in the advertising media? Chiropr Osteopat, 15, 7. doi.org/10.1186/1746-1340-15-7
Deyo, R. A., Loeser, J. D., & Bigos, S. J. (1990). Herniated lumbar intervertebral disk. Ann Intern Med, 112(8), 598-603. doi.org/10.7326/0003-4819-112-8-598
Gallucci, M., Puglielli, E., Splendiani, A., Pistoia, F., & Spacca, G. (2005). Degenerative disorders of the spine. Eur Radiol, 15(3), 591-598. doi.org/10.1007/s00330-004-2618-4
Katz, J. N., Zimmerman, Z. E., Mass, H., & Makhni, M. C. (2022). Diagnosis and Management of Lumbar Spinal Stenosis: A Review. JAMA, 327(17), 1688-1699. doi.org/10.1001/jama.2022.5921
Back problems and discomfort symptoms are a common ailment that many types of healthcare providers diagnose and treat it. Can knowing a little about what each back pain specialist does and what they have to offer help in choosing a provider?
Back Pain Specialists
Nowadays individuals have options for treating back pain. Primary healthcare providers, general practitioners, pediatricians, and emergency room workers are usually the first to examine the injury or problem. If they are unable to properly diagnose or treat the injury, they will refer the individual to a specialist. Specialists include:
Osteopaths
Chiropractors
Orthopedists
Rheumatologists
Neurologists
Neurosurgeons.
They specialize in chronic conditions and diseases like arthritis or problems like herniated discs. Complementary and alternative providers treat individuals solely or with help from a care team. They look at the whole body and focus on improving overall function.
Family and General Practitioners
When neck or back pain begins a regular doctor that’s usually a family or general practitioner/GP or primary care provider PCP is a recommended place to start. They will:
Order diagnostic tests.
Recommend exercises and stretches.
Prescribe medication.
Refer the patient to a physical therapist or other back pain specialist.
However, studies suggest general providers can be uninformed and slow to adopt new back treatments. (Paul B. Bishop, Peter C. Wing. 2006) It is recommended to research possible treatment options, ask a lot of questions during an appointment, and ask or request a referral to a specialist.
Pediatricians
Pediatricians diagnose and treat children. They cover a wide range of issues including back problems and injuries. As with a general practitioner or primary care provider, a child’s pediatrician is the place to start. Depending on the child’s needs, they’ll refer them to the proper specialist.
Emergency Healthcare Providers
When there is serious neck or back trauma, individuals need to go to the emergency room. Trauma can include automobile collisions, sports accidents, work accidents, and/or personal home accidents. Someone with a possible spinal injury should not be moved. (W Yisheng, et al., 2007) Go to the ER if there is back pain with loss of bowel or bladder control, or the legs become progressively weaker. These are symptoms of an emergency condition known as cauda equina syndrome. (American Association of Neurological Surgeons. 2023)
Orthopedists
Orthopedists and orthopedic surgeons treat the musculoskeletal system, which includes:
Muscles
Bones
Joints
Connective tissues
Cartilage
Common orthopedic issues include:
Repetitive stress injuries
Sports injuries
Bursitis
Tendonitis
Ruptured discs
Nerve impingement
Scoliosis
Osteoporosis
Osteoarthritis
Orthopedics can overlap with other specialties. As orthopedists and rheumatologists both treat arthritis and orthopedic surgeons and neurosurgeons do some of the same procedures that include spinal fusions and discectomies.
Rheumatologists
A rheumatologist treats autoimmune, inflammatory, and musculoskeletal conditions that can include different types of arthritis, lupus, and Sjogren’s syndrome. A primary care provider may refer a patient to a rheumatologist if they have symptoms that include:
Sacroiliitis – inflammation of the sacroiliac joint at the base of the spine.
Axial spondylosis – a form of spinal arthritis.
Axial spondylosis – spinal arthritis that causes the bones to fuse together.
Rheumatologists can also treat spinal stenosis or advanced osteoarthritis as they overlap with orthopedists.
Neurologists
A neurologist specializes in the function of the nervous system. They treat disorders of the brain, spinal cord, and nerves that include:
Parkinson’s disease
Multiple sclerosis
Alzheimer’s disease
Chronic back or neck pain
They are experts in the origins of pain. (David Borsook. 2012) However, a neurologist does not perform spine surgery.
Neurosurgeons
A neurosurgeon specializes in nervous system surgical procedures that include the brain, spine, and spinal cord. However, neurosurgeons do not provide overall treatment for back pain because they are usually the last to be seen after exhausting all other treatment options.
Osteopaths
An osteopath is a licensed physician who practices medicine using conventional treatments and osteopathic manipulative medicine. They have the same education as an MD plus 500 hours of musculoskeletal system studies. (National Library of Medicine. 2022) They take the same exams and are licensed as an MD. Many osteopaths are primary care providers. For back pain, they will focus on:
Posture rehabilitation and training.
Stretching
Therapeutic massage
Spinal manipulation
The goal is to relieve pain and muscle tension, increase mobility, and improve musculoskeletal function.
Physiatrists
Physiatrists are holistic providers that focus on physical function. They can be thought of as a primary care provider plus a physical therapist. These back pain specialists provide rehabilitation for various types of conditions and injuries including:
Back pain
Sports injuries
Stroke
Often they will coordinate a team of specialists to develop a targeted treatment plan.
Chiropractor
Chiropractic is a hands-on alternative medicine. The goal is to restore neuromusculoskeletal function by realigning the spine to its proper form. They do this with spinal manipulations, non-surgical mechanical decompression, traction, and massage techniques. (Michael Schneider, et al., 2016)
The purpose of most chiropractic adjustments is to relax and retrain tight muscles and increase flexibility.
Chiropractic helps to relieve stiff muscles and restore range of motion.
Individuals may not be referred to a chiropractor if they:
Have loose-joints
Have connective tissue problems or conditions.
Have osteoporosis/thinning bones
All types of back pain specialists provide various forms of therapy that may be able to help.
Spinal Decompression in Depth
References
Bishop, P. B., & Wing, P. C. (2006). Knowledge transfer in family physicians managing patients with acute low back pain: a prospective randomized control trial. The spine journal : official journal of the North American Spine Society, 6(3), 282–288. doi.org/10.1016/j.spinee.2005.10.008
Yisheng, W., Fuying, Z., Limin, W., Junwei, L., Guofu, P., & Weidong, W. (2007). First aid and treatment for cervical spinal cord injury with fracture and dislocation. Indian journal of orthopaedics, 41(4), 300–304. doi.org/10.4103/0019-5413.36991
Schneider, M., Murphy, D., & Hartvigsen, J. (2016). Spine Care as a Framework for the Chiropractic Identity. Journal of chiropractic humanities, 23(1), 14–21. doi.org/10.1016/j.echu.2016.09.004
Individuals with fixed sagittal imbalance, a condition where the normal curve of the lower spine is greatly reduced or absent altogether that can cause pain and difficulty balancing. Can chiropractic treatment, physical therapy, and exercise help improve the condition?
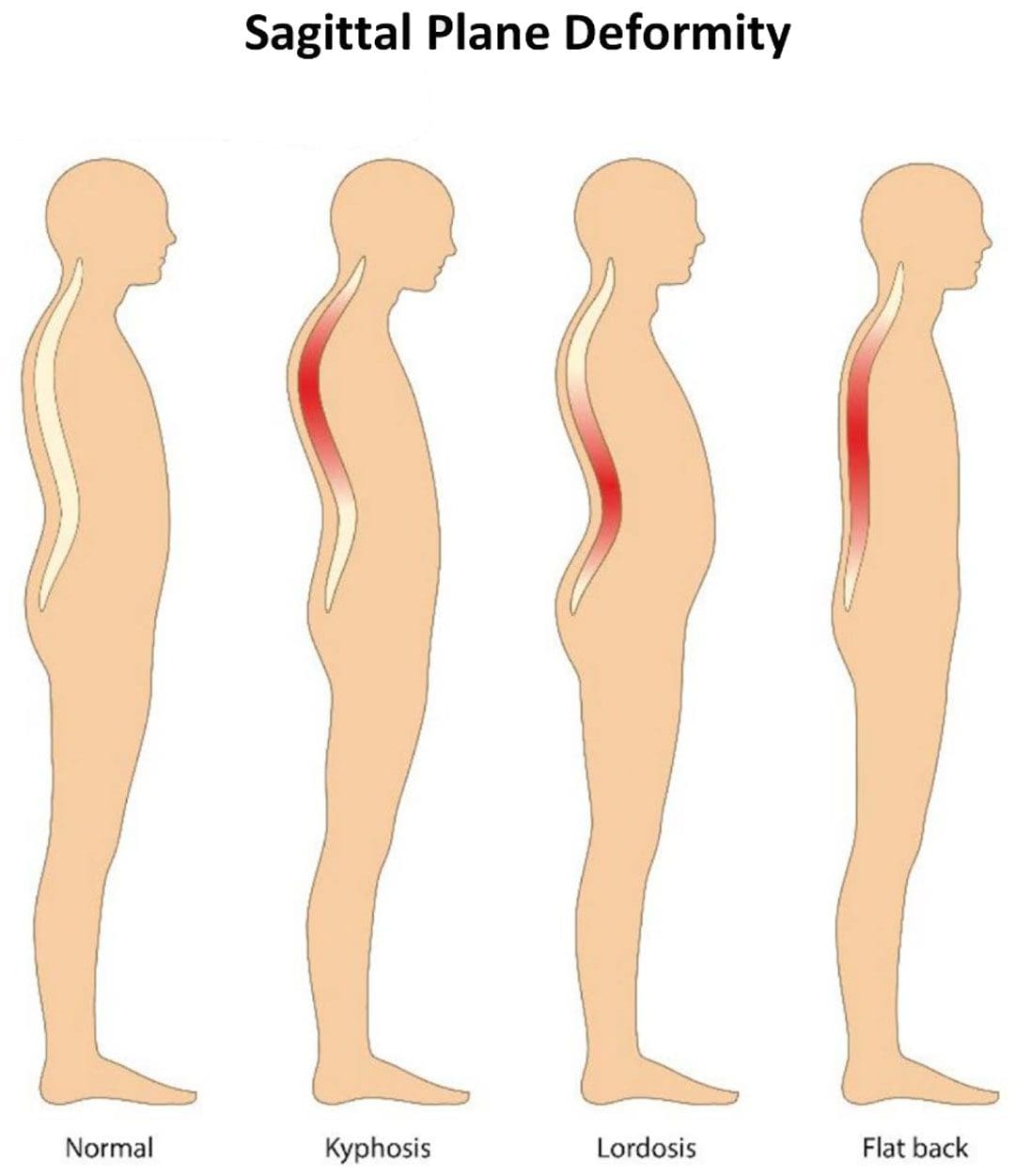
Fixed Sagittal Imbalance
The condition is commonly known as flat back syndrome and can be present at birth or can happen as a result of surgery or a medical condition.
Individuals with flat back syndrome position their head and neck too far forward.
A major symptom is difficulty standing for long periods of time.
Symptoms
The spine has two curves. The lumbar spine in the lower back and cervical spine in the neck curve inward. The thoracic spine in the upper back curves outward. The curves are part of the spine’s natural alignment. They help the body balance and maintain the center of gravity.
If these curves begin to disappear the body can have trouble and difficulty standing up straight.
The loss of curvature causes the head and neck to pitch forward, making it hard to walk and do regular normal activities.
A chiropractor and/or physical therapist can recommend exercises and other forms of treatment. (Won-Moon Kim, et al., 2021)
Life-Changing Chiropractic Relief
References
Columbia University Irving Medical Center. Flatback syndrome.
National Health Service. Common posture mistakes and fixes.
Lee, B. H., Hyun, S. J., Kim, K. J., Jahng, T. A., Kim, Y. J., & Kim, H. J. (2018). Clinical and Radiological Outcomes of Posterior Vertebral Column Resection for Severe Spinal Deformities. Journal of Korean Neurosurgical Society, 61(2), 251–257. doi.org/10.3340/jkns.2017.0181
Kim, W. M., Seo, Y. G., Park, Y. J., Cho, H. S., & Lee, C. H. (2021). Effect of Different Exercise Types on the Cross-Sectional Area and Lumbar Lordosis Angle in Patients with Flat Back Syndrome. International journal of environmental research and public health, 18(20), 10923. doi.org/10.3390/ijerph182010923
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine