Back Clinic Conditions Treated. Chronic Pain, Auto Accident Care, Back Pain, Low Back Pain, Back Injuries, Sciatica, Neck Pain, Work Injuries, Personal Injuries, Sports Injuries, Migraine Headaches, Scoliosis, Complex Herniated Discs, Fibromyalgia, Wellness & Nutrition, Stress Management, and Complex Injuries.
At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we are focused on treating patients after debilitating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities.
If Dr. Alex Jimenez feels you need other treatment, then you will be referred to a clinic or Physician that is best suited for you. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, and premiere rehabilitation providers to bring El Paso the top clinical treatments to our community. Providing the top non-invasive protocols is our priority. Clinical insight is what our patients demand in order to give them the appropriate care required. For answers to any questions you may have please call Dr. Jimenez at 915-850-0900
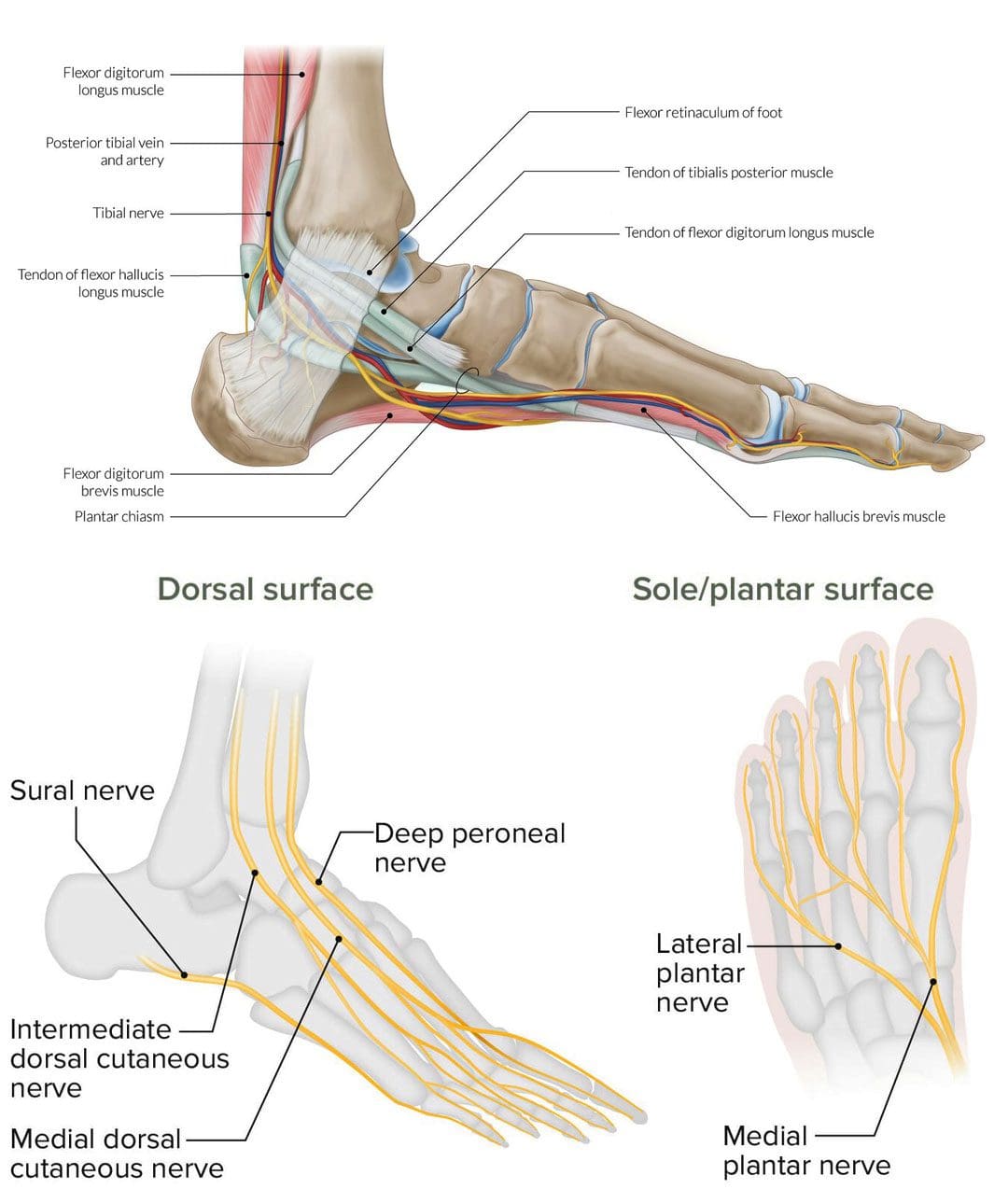
Individuals that experience nerve pain in the foot could be caused by a number of different conditions, can recognizing the most common causes help in developing an effective treatment plan?
Nerve Pain In The Foot
These sensations can feel like a burning, shooting, electrical, or stabbing pain and can happen while in motion or at rest. It can occur on the top of the foot or through the arch. The area closest to the nerve may be sensitive to the touch. A number of different conditions can cause nerve pain in the foot, including:
Morton’s neuroma
Pinched nerve
Tarsal tunnel syndrome
Diabetic peripheral neuropathy
Herniated disc
Morton’s Neuroma
Morton’s neuroma involves the nerve that runs between the third and fourth toes, but can sometimes occur between the second and third toes becoming thicker. Typical symptoms include a burning or shooting pain in the area, usually while walking. (Nikolaos Gougoulias, et al., 2019) Another common symptom is the sensation of pressure beneath the toes like the sock is bunched up underneath. Treatments can include:
Arch supports
Cortisone injections to decrease swelling
Footwear modifications – can include lifts, orthotics combined with metatarsal pads, and rocker soles, to provide cushion where needed.
Things that increase the risk of developing the condition include:
Regularly wearing high-heels – the condition occurs more frequently in women.
Shoes that are too tight.
Participating in high-impact sports like running.
Having flat feet, high arches, bunions, or hammertoes.
Pinched Nerve
A pinched nerve can feel like shooting or burning pain. Nerve entrapment can occur in various regions of the foot or the area on top of the foot may feel sensitive. Causes can be caused by: (Basavaraj Chari, Eugene McNally. 2018)
Trauma that causes swelling.
Blunt impact.
Tight shoes.
Treatment can include:
Massage
Physical therapy
Rest
Footwear modifications
Anti-inflammatories.
Things that increase the risk of developing a pinched nerve in the foot include:
Poor-fitting footwear.
Repetitive stress injury.
Trauma to the foot.
Obesity.
Rheumatoid arthritis.
Tarsal Tunnel Syndrome
Another type of nerve entrapment is tarsal tunnel syndrome. Tarsal tunnel syndrome is “anything that produces compression on the posterior tibial nerve.” (American College of Foot and Ankle Surgeons. 2019) The tibial nerve is located near the heel. Symptoms include numbness and foot cramps, burning, tingling, or shooting sensations that often radiate from the instep/arch. Both can worsen while the foot is at rest, like when sitting or sleeping. Treatment can consist of:
Placing padding in the shoe where the foot is being compressed to relieve the pain.
Custom foot orthotics.
Cortisone shots or other anti-inflammatory treatments.
Surgery may be necessary to release the nerve.
Conditions that compress the tibial nerve and can lead to tarsal tunnel syndrome include:
Flat feet
Fallen arches
Ankle sprain
Diabetes
Arthritis
Varicose veins
Bone spurs
Diabetic Peripheral Neuropathy
Long-term high blood sugar/glucose associated with diabetes can lead to a form of nerve damage known as peripheral neuropathy. (Centers for Disease Control and Prevention. 2022) Neuropathy pain feels like burning or shooting pain, or the sensation of walking on bubble wrap that usually shows up overnight. The pain can come and go as well as a gradual loss of feeling in the feet that begins in the toes and moves up the foot. It’s estimated that around half of individuals with diabetes will eventually develop neuropathy. (Eva L. Feldman, et al., 2019) Treatments can include:
Physical therapy massage to increase circulation.
Topical treatments with capsaicin.
Vitamin B.
Blood sugar management.
Alpha lipoic acid.
Medication.
Individuals with diabetes have an increased risk of developing peripheral neuropathy if:
Blood sugar is not well-controlled.
Diabetes has been present for many years.
Kidney disease.
Smoke.
Overweight or obese.
Herniated Disc
Nerve pain in the foot can be caused by spinal issues. A herniated disc in the lower back can irritate and compress the nerves, causing pain that radiates down the leg and foot. Additional symptoms usually include muscle weakness in the legs and/or numbness and tingling. Most herniated discs don’t require surgery and get better with conservative treatment. (Wai Weng Yoon, Jonathan Koch. 2021) If symptoms don’t improve or worsen, a healthcare provider may recommend surgery. Herniated discs are most common in young and middle-aged adults. Increased chances of developing a herniated disc can come from:
Degenerative changes in the spine from normal age wear and tear.
Physically demanding job.
Lifting incorrectly.
Overweight or obese.
Genetic predisposition – family history of herniated discs.
Spinal Stenosis
Spinal stenosis occurs when the spaces in the spine begin to narrow, creating pressure on the spinal cord and nerve roots. It is usually caused by wear and tear on the spine as the body ages. Stenosis in the lower back can cause burning pain in the buttocks and leg. As it progresses pain can radiate into the feet along with numbness and tingling. Conservative treatment consists of physical therapy exercises and non-steroidal anti-inflammatory medications/NSAIDs. (Jon Lurie, Christy Tomkins-Lane. 2016) Cortisone injections can be beneficial and if the condition worsens, surgery may be an option. Risk factors include:
Physical trauma – after surgery or an automobile or sports accident.
Certain cancer, antiviral medications, or antibiotics.
Complex regional pain syndrome.
Tumors that irritate and/or compress a nerve.
Liver or kidney disease.
Infectious diseases – Lyme disease complications or viral infections.
Nerve pain in the foot is definitely a reason to see a healthcare provider. Early diagnosis can help prevent symptom progression and future problems. Once the cause of the pain has been identified, the healthcare team can work together to develop a personalized treatment plan to release compressed nerves and restore mobility and function. See a healthcare provider right away if the pain and symptoms worsen, or if there are difficulties standing or walking.
Chiropractic After Accidents and Injuries
References
Gougoulias, N., Lampridis, V., & Sakellariou, A. (2019). Morton’s interdigital neuroma: instructional review. EFORT open reviews, 4(1), 14–24. doi.org/10.1302/2058-5241.4.180025
Chari, B., & McNally, E. (2018). Nerve Entrapment in Ankle and Foot: Ultrasound Imaging. Seminars in musculoskeletal radiology, 22(3), 354–363. doi.org/10.1055/s-0038-1648252
Feldman, E. L., Callaghan, B. C., Pop-Busui, R., Zochodne, D. W., Wright, D. E., Bennett, D. L., Bril, V., Russell, J. W., & Viswanathan, V. (2019). Diabetic neuropathy. Nature reviews. Disease primers, 5(1), 42. doi.org/10.1038/s41572-019-0097-9
Yoon, W. W., & Koch, J. (2021). Herniated discs: when is surgery necessary?. EFORT open reviews, 6(6), 526–530. doi.org/10.1302/2058-5241.6.210020
Lurie, J., & Tomkins-Lane, C. (2016). Management of lumbar spinal stenosis. BMJ (Clinical research ed.), 352, h6234. doi.org/10.1136/bmj.h6234
Staff, N. P., & Windebank, A. J. (2014). Peripheral neuropathy due to vitamin deficiency, toxins, and medications. Continuum (Minneapolis, Minn.), 20(5 Peripheral Nervous System Disorders), 1293–1306. doi.org/10.1212/01.CON.0000455880.06675.5a
Temporomandibular joint disorder causes pain and jaw locking that can be worsened with certain activities. How individuals can manage and prevent flare-ups by learning what not to do to worsen the condition?
What Not To Do Temporomandibular Joint Disorder
Tenderness, aching, pain, and jaw locking are symptoms of temporomandibular joint disorder or TMJ. The temporomandibular joint connects the jaw to the skull. It is used daily for eating, drinking, and talking. It is a small disc in the joint that allows the jaw bones to slip and slide correctly. With TMJ, the disc shifts out of place, leading to clicking, snapping, and limited jaw movement. It can also cause pain in the jaw and face, neck pain, and headaches, and the muscles around the jaw and neck can become sore and/or go into spasm. Any type of activity that stresses or overworks the joint can trigger a flare-up and worsen TMJ symptoms. (Schiffman E, et al. 2014) This article looks at avoiding activities that make TMJ worse and what not to do to help keep TMJ symptoms in check.
Chewing Gum
Gum chewing is not recommended for individuals with TMJ.
The jaw is one of the most used joints in the body.
Limiting excessive use alleviates pressure allowing the joints and muscles to rest.
Resting sore muscles and joints is the first step in injury recovery.
Eating Chewy and Hard Foods
Chewy and hard foods make the jaw have to work overtime.
Avoid eating hard foods like chewy candies, hard and chewy breads, vegetables like corn on the cob, and fruits like apples.
These foods can place excessive stress on the jaw, and prevent the joint from properly resting and healing.
Chewing Only On One Side
Many individuals chew their food on only one side of the mouth.
This can stress out one side of the temporomandibular joint and surrounding muscles, leading to pain and dysfunction. (Urbano Santana-Mora, et al., 2013)
Stay aware of chewing habits and make sure to utilize both sides of the mouth.
Individuals with dental issues or tooth pain are recommended to see a dentist.
Non-Functional Jaw Activities
Going through each day, individuals tend to do things unconsciously or out of habit.
For example, individuals:
Reading or writing might chew on a pen or pencil.
Bite their nails or chew on the inside of their mouth while watching TV or internet browsing.
These activities can place stress on the joint, worsen the condition, and extend the healing process.
Resting on The Chin
Individuals will rest their jaw in their hands while studying, on social media, or watching TV.
This position can be comfortable, but it can affect the jaw.
This position can build pressure against the side of the jaw and push against the joint, causing the disc to shift out of place affecting how the jaw opens and closes.
Breaking the chin resting habit can allow the joint to relax and heal correctly.
Teeth Clenching
Bruxism is the medical term for clenching the teeth.
This can occur during the day or during sleep.
Teeth clenching is often brought on by stress and can place incredible pressure on the jaw’s muscles and worsen TMJ.
A dentist can prescribe a mouth guard to be worn while sleeping to protect the teeth from excessive clenching. (Miriam Garrigós-Pedrón, et al., 2019)
Slouching
The function of the jaw is closely related to body posture.
The jaw operates optimally when the head is above the cervical spine and the posture is upright.
Slouching can change how the jaw muscles work and the way the jaw opens and closes.
Part of physical therapy for TMJ is working on posture adjustments and training.
This can involve strengthening the back and shoulder muscles and setting up posture reminders.
Sitting and standing correctly can keep the jaw operating properly.
Postponing Treatment
Many with musculoskeletal issues and symptoms wait for the pain to go away.
Individuals having problems with their jaw should not wait to get treatment.
TMJ has a positive rate of recovery with conservative treatment, which is all the more reason to seek treatment. (G Dimitroulis. 2018)
A dentist or healthcare provider can provide an accurate diagnosis if TMJ is suspected.
Individuals can benefit from visiting a physical therapist to learn exercises and strategies to self-treat the condition. (Yasser Khaled, et al., 2017)
Treatment
Treatment can involve:
Initial treatment focuses on pain relief and jaw function opens and closes improvement.
A guard can help with night teeth grinding/bruxism.
Anti-inflammatory treatments.
In severe cases, surgery may be recommended to correct the problem, as a last resort. (Meghan K Murphy, et al., 2013)
Follow recommendations on what not to do and avoid certain activities.
Quick Patient Initiation
References
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J. P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., Michelotti, A., Brooks, S. L., Ceusters, W., Drangsholt, M., Ettlin, D., Gaul, C., Goldberg, L. J., Haythornthwaite, J. A., Hollender, L., Jensen, R., … Orofacial Pain Special Interest Group, International Association for the Study of Pain (2014). Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. Journal of oral & facial pain and headache, 28(1), 6–27. doi.org/10.11607/jop.1151
Santana-Mora, U., López-Cedrún, J., Mora, M. J., Otero, X. L., & Santana-Penín, U. (2013). Temporomandibular disorders: the habitual chewing side syndrome. PloS one, 8(4), e59980. doi.org/10.1371/journal.pone.0059980
Garrigós-Pedrón, M., Elizagaray-García, I., Domínguez-Gordillo, A. A., Del-Castillo-Pardo-de-Vera, J. L., & Gil-Martínez, A. (2019). Temporomandibular disorders: improving outcomes using a multidisciplinary approach. Journal of multidisciplinary healthcare, 12, 733–747. doi.org/10.2147/JMDH.S178507
Dimitroulis G. (2018). Management of temporomandibular joint disorders: A surgeon’s perspective. Australian Dental Journal, 63 Suppl 1, S79–S90. doi.org/10.1111/adj.12593
Khaled Y, Quach JK, Brennan MT, NapeÑas JJ. Outcomes after physical therapy for the treatment of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol, 2017;124(3: e190. doi:10.1016/j.oooo.2017.05.477
Abouelhuda, A. M., Khalifa, A. K., Kim, Y. K., & Hegazy, S. A. (2018). Non-invasive different modalities of treatment for temporomandibular disorders: a review of the literature. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 44(2), 43–51. doi.org/10.5125/jkaoms.2018.44.2.43
Murphy, M. K., MacBarb, R. F., Wong, M. E., & Athanasiou, K. A. (2013). Temporomandibular disorders: a review of etiology, clinical management, and tissue engineering strategies. The International journal of oral & maxillofacial implants, 28(6), e393–e414. doi.org/10.11607/jomi.te20
Can chiropractic treatment protocols diagnose what’s causing head pressure in individuals, and provide effective treatment?
Head Pressure
Head pressure can have various causes and symptoms that affect different areas depending on whether the cause is a headache, allergies, injury, illness, or disease. The location of the pressure or pain can help a doctor of chiropractic determine the cause.
The underlying factor is usually not life-threatening, but the pressure that has built can be the result of serious conditions like a head injury or brain tumor.
Chiropractic care, which includes a combination of spinal manipulation, active and passive exercises, and massage, is often used for headache management and prevention. (Moore Craig, et al., 2018)
Chiropractic therapy is often sought out for tension and cervicogenic headaches, migraines, and each responds differently to the treatment.
The Head
The head is made up of a complex system of lobes, sinuses/channels, blood vessels, nerves, and ventricles. (Thau L, et al., 2022)
The pressure of these systems is regulated and any disruption to this balance can be noticeable.
Diagnosis can be difficult to figure out what is causing discomfort or head pressure.
Pain, pressure, irritability, and nausea are all symptoms that can occur with headaches. (Rizzoli P, Mullally W. 2017)
Head pressure can also occur only at times when standing up, bending down to pick up an object, or otherwise changing posture in some way that blood pressure is affected.
Chiropractic Treatment
The Injury Medical team will develop a personalized treatment plan to help relieve pressure symptoms through a multidisciplinary approach that can include. (Moore Craig, et al., 2018)
Moore, C., Leaver, A., Sibbritt, D., & Adams, J. (2018). The management of common recurrent headaches by chiropractors: a descriptive analysis of a nationally representative survey. BMC neurology, 18(1), 171. doi.org/10.1186/s12883-018-1173-6
Schizodimos, T., Soulountsi, V., Iasonidou, C., & Kapravelos, N. (2020). An overview of the management of intracranial hypertension in the intensive care unit. Journal of Anesthesia, 34(5), 741–757. doi.org/10.1007/s00540-020-02795-7
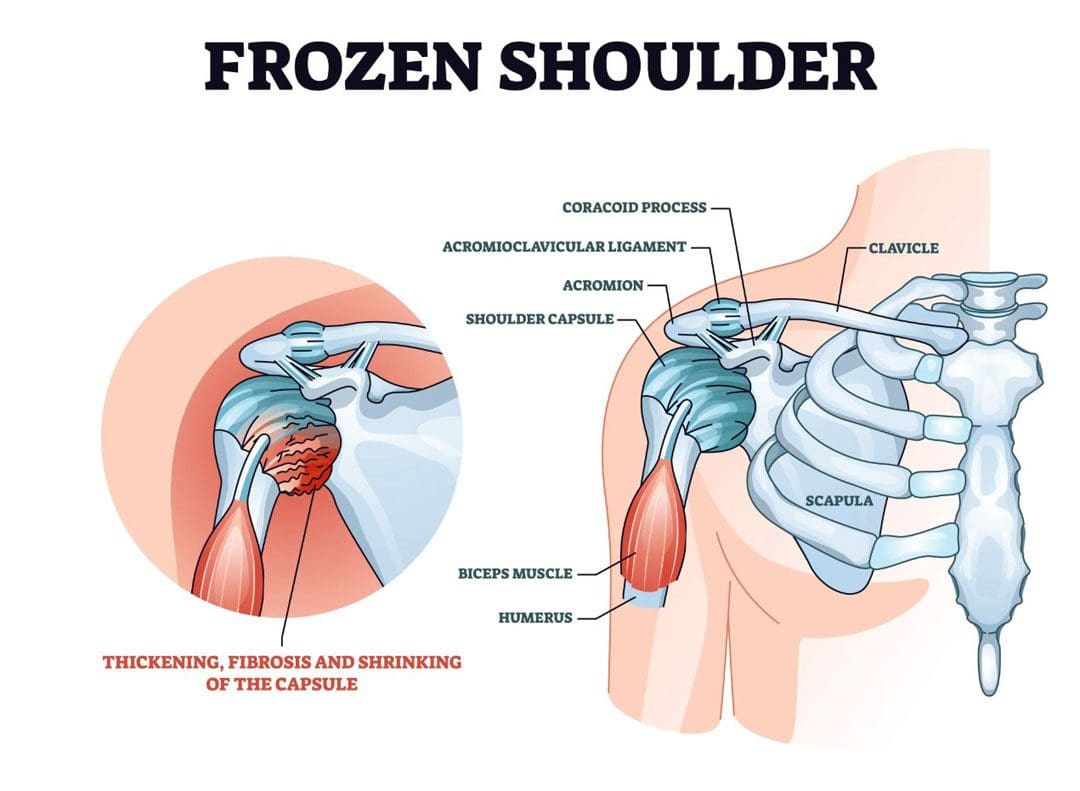
Stiffness and pain developing in the shoulder could be adhesive capsulitis, (frozen shoulder), a condition in the shoulder’s ball-and-socket joint/glenohumeral joint. It usually develops over time and limits the functional use of the arm. The pain and tightness restrict arm movement, and the duration of symptoms can persist for 12-18 months. The cause is often unknown, but it is more common in individuals over 40, individuals with diabetes, thyroid disease, and cardiac conditions have an increased risk of developing the condition, and women tend to develop the condition more than men. Chiropractic treatment can be effective at relieving pain and expediting recovery.
Stiffness and Pain
The shoulder joint allows more movement than any other joint in the body. A frozen shoulder causes the capsule surrounding the shoulder joint to contract and form scar tissue. The capsule contraction and the formation of adhesions cause the shoulder to become stiff, restrict movement, and cause pain and discomfort symptoms.
Stages
The progression is marked by three stages:
Freezing
Stiffness and pain begin to restrict motion.
Frozen
Movement and motion are severely restricted.
Thawing
The shoulder starts to loosen up.
It can take years to fully resolve symptoms.
In mild cases, a frozen shoulder can go away on its own but that does not mean that it is truly healed and correctly aligned.
Even in mild cases seeking treatment is recommended, rather than just waiting for it to go away.
Symptoms
Limited range of motion.
Stiffness and tightness.
Dull or aching pain throughout the shoulder.
Pain can radiate into the upper arm.
Pain can be triggered by the smallest movements.
The symptoms are not always due to weakness or injury, but actual joint stiffness.
Causes
Most frozen shoulders occur with no injury or discernible cause but the condition is often linked to a systemic condition or one that affects the entire body.
Age and Gender
Frozen shoulder most commonly affects individuals between the ages of 40 to 60, and is more common in women than in men.
Endocrine Disorders
Individuals with diabetes have an increased risk of developing a frozen shoulder.
Other endocrine abnormalities like thyroid problems can also lead to the development of this condition.
Shoulder Trauma and/or Surgery
Individuals who sustain a shoulder injury, or undergo surgery on the shoulder can develop a stiff and painful joint.
When injury or surgery is followed by prolonged immobilization/resting the arm, the risk of developing a frozen shoulder increases.
Other Systemic Conditions
Several systemic conditions such as heart disease have also been associated with an increased risk of developing the condition and can include:
High cholesterol
Adrenal disease
Heart and lung disease
Parkinson’s disease
Stiffness and pain can also be associated with damage to the joint from injuries or other shoulder problems that include:
A frozen shoulder associated with any of these causes is considered secondary.
Treatment
A diagnosis is made by observing the range of motion in the shoulder, considering the two types:
Active Range
This is how far an individual can move a body part on their own.
Passive Range
This is how far another person like a therapist or doctor can move the body part.
Therapies
Chiropractic, massage, and physical therapy involve stretches, realignment, and exercises to relieve pain symptoms and restore mobility and function.
Usually, strength is not affected by a frozen shoulder but a chiropractor may want to strengthen the surrounding muscles to better support the shoulder and prevent worsening the injury or causing a new injury.
Anti-inflammatory medications and corticosteroid injections may help manage pain symptoms.
Getting a diagnosis and treatment during the freezing stage can keep the condition from progressing and expedite recovery time.
Enhancing Health: Evaluation and Treatment
References
Brun, Shane. “Idiopathic frozen shoulder.” Australian Journal of general practice vol. 48,11 (2019): 757-761. doi:10.31128/AJGP-07-19-4992
Chan, Hui Bin Yvonne, et al. “Physical therapy in the management of frozen shoulder.” Singapore medical journal vol. 58,12 (2017): 685-689. doi:10.11622/smedj.2017107
Cho, Chul-Hyun, et al. “Treatment Strategy for Frozen Shoulder.” Clinics in orthopedic surgery vol. 11,3 (2019): 249-257. doi:10.4055/cios.2019.11.3.249
Duzgun, Irem, et al. “Which method for frozen shoulder mobilization: manual posterior capsule stretching or scapular mobilization?.” Journal of Musculoskeletal & neuronal interactions vol. 19,3 (2019): 311-316.
Jain, Tarang K, and Neena K Sharma. “The effectiveness of physiotherapeutic interventions in the treatment of frozen shoulder/adhesive capsulitis: a systematic review.” Journal of back and musculoskeletal rehabilitation vol. 27,3 (2014): 247-73. doi:10.3233/BMR-130443
Kim, Min-Su, et al. “Diagnosis and treatment of calcific tendinitis of the shoulder.” Clinics in shoulder and elbow vol. 23,4 210-216. 27 Nov. 2020, doi:10.5397/cise.2020.00318
Millar, Neal L et al. “Frozen shoulder.” Nature reviews. Disease primers vol. 8,1 59. 8 Sep. 2022, doi:10.1038/s41572-022-00386-2
Lying down on the couch or bed when the lower leg seizes with intense sensations and pain that doesn’t stop, and the muscle could be hard to the touch. When trying to move the leg, it feels paralyzed. Nocturnal leg cramps, called muscle spasms or Charley horses, occur when one or more leg muscles tighten involuntarily. Individuals can be awake or asleep when a leg cramp strikes. Chiropractic treatment, decompression, and massage therapies can help relieve symptoms, stretch and relax the muscles, and restore function and health.
Nocturnal Leg Cramps
Nocturnal leg cramps most often affect the gastrocnemius/calf muscle. However, they can also affect the muscles in the front of the thigh/quadriceps and the back of the thigh/hamstrings.
Often, the tight muscle relaxes in less than 10 minutes.
The leg and area can feel sore and tender afterward.
Frequent calf cramps at night can cause sleep problems.
Nocturnal leg cramps are more common among women and older adults.
Causes
There are no known exact cause/s, making most cases idiopathic. However, there are known factors that can increase the risk. These can include:
Prolonged Sitting and Position
Sitting with the legs crossed or the toes pointed for long periods shortens/pulls the calf muscles, which can cause cramping.
Prolonged Standing and Posture
Individuals standing for long periods are likelier to experience nocturnal cramps from the stressed muscles.
Muscle Overexertion
Too much exercise can create an overworked muscle and can contribute to cramps.
Muscles need to be stretched regularly to function correctly.
Lack of physical activity for long periods weakens the muscles, making them more susceptible to injury.
Shortening The Tendons
The tendons, which connect muscles and bones, shorten naturally over time.
Without stretching, this could lead to cramping.
Cramps may be related to foot position when sleeping, with the feet and toes extending away from the body, known as plantar flexion.
This shortens the calf muscles, making them more susceptible to cramping.
Leg cramps at night are unlikely a sign of a more serious medical condition, but they are associated with the following conditions:
Musculoskeletal disorders.
Structural issues – flat feet or spinal stenosis.
Metabolic disorders like diabetes.
Pregnancy.
Medications – statins and diuretics.
Neurological disorders, like motor neuron disease or peripheral neuropathy.
Neurodegenerative disorders.
Liver, kidney, and thyroid conditions.
Cardiovascular conditions.
Chiropractic and Physical Therapy
Rehabilitation with chiropractic, massage, and physical therapy depends on the severity of the injury and condition. A chiropractic treatment plan can include the following:
Calf muscle stretching.
Targeted Stretch Exercises.
Progressive calf stretching exercises – a regular stretching and flexibility program will increase the range of motion and prevent future calf injuries.
Foam rolling – gentle self-massage with a foam roller can help reduce spasms and improve blood circulation.
Percussive massage.
Muscle strengthening exercises will build muscle strength and coordination to prevent future strain injuries.
At-home therapy can include:
Maintain Hydration
Fluids allow for normal muscle function.
Individuals may need to adjust how much fluid is drunk based on weather, age, activity level, and medications.
Change Sleeping Position
Individuals should avoid sleeping in positions in which the feet are pointing downward.
Try sleeping on the back with a pillow behind the knees.
Self Massage
Massaging the affected muscles will help them relax.
Use one or both hands or a massage gun to knead and loosen the muscles gently.
Stretching
Various stretches will maintain the treatment, help keep the muscles relaxed and retrain the muscles.
Stationary Cycle
A few minutes of easy pedaling can help loosen the leg muscles before bed.
Walking on the Heels
This will activate the muscles on the other side of the calf, allowing the calves to relax.
Supportive Footwear
Poor footwear can aggravate issues with the nerves and muscles in the feet and legs.
Orthotics may help.
Heat Application
Heat can soothe tight muscles and increases blood flow to the area.
Apply a hot towel, water bottle, heating pad, or muscle topical cream to the affected area.
A warm bath or shower (if available, shower massage setting) can also help.
Sciatica Secrets Revealed
References
Allen, Richard E, and Karl A Kirby. “Nocturnal leg cramps.” American family physician vol. 86,4 (2012): 350-5.
Butler, J V et al. “Nocturnal leg cramps in older people.” Postgraduate medical journal vol. 78,924 (2002): 596-8. doi:10.1136/pmj.78.924.596
Garrison, Scott R et al. “Magnesium for skeletal muscle cramps.” The Cochrane Database of systematic reviews vol. 2012,9 CD009402. Sep 12, 2012, doi:10.1002/14651858.CD009402.pub2
Giuffre BA, Black AC, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2023 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK482431/
Handa, Junichi, et al. “Nocturnal Leg Cramps and Lumbar Spinal Stenosis: A Cross-Sectional Study in the Community.” International Journal of general medicine vol. 15 7985-7993. Nov 1 2022, doi:10.2147/IJGM.S383425
Hsu D, Chang KV. Gastrocnemius Strain. [Updated 2022 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK534766/
Mayo Clinic Staff. (2019). Night leg cramps. mayoclinic.org/symptoms/night-leg-cramps/basics/causes/sym-20050813
Monderer, Renee S et al. “Nocturnal leg cramps.” Current Neurology and Neuroscience report vol. 10,1 (2010): 53-9. doi:10.1007/s11910-009-0079-5
Upper and middle/mid-back pain and/or pain between the shoulder blades is common for individuals who spend long hours sitting or standing. Stress, tension, and repetitive movements can cause middle-back trigger points to develop. Symptoms occur anywhere from the neck’s base to the bottom of the rib cage. Trigger point development and reoccurrence can contribute to chronic upper and middle back pain. Injury Medical Chiropractic and Functional Medicine Clinic can release, relieve and help prevent trigger points through various therapies and treatment plans.
Middle Back Trigger Points
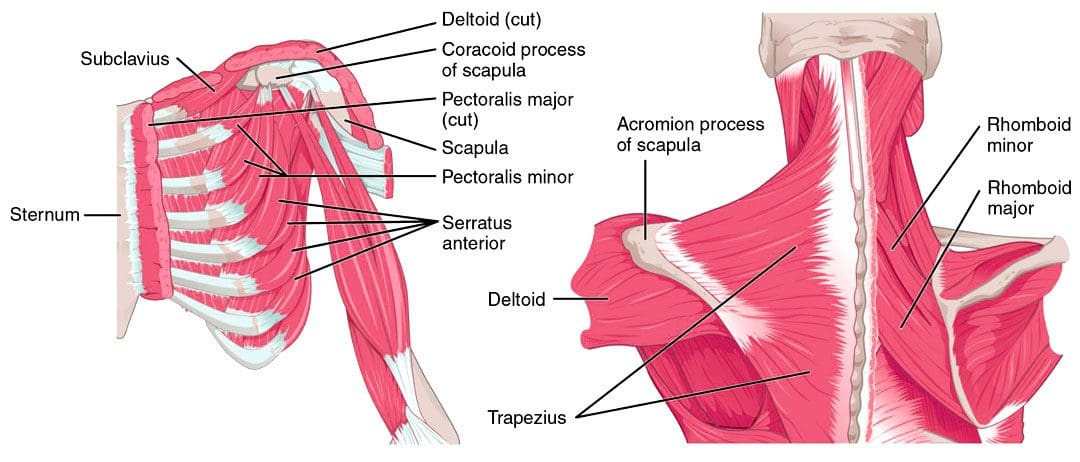
The ribs attach to the sternum and adhere to and wrap around the back. Pain and sensation symptoms can radiate to other places where the nerve travels if a nerve in this area is pinched, irritated, or injured. The muscle groups of the chest region also have a significant role in middle back trigger point development. Tension in the chest muscles can overload the muscles of the mid-back region, causing tightness. This happens to individuals that release the trigger points in the mid-back muscles but fail to address the trigger points in the chest muscles, causing reactivation that could worsen the injury. Three muscle groups can cause trigger point referred pain between the shoulder blades include:
Rhomboid Trigger Points Between the Shoulder Blades
The Rhomboid muscle group is found in the mid-back region, between the shoulder blades.
These muscles attach along the spine and run diagonally downward to connect to the inside of the shoulder blade.
The contraction causes the shoulder blades to retract and rotate.
Trigger points only cause pain in the region of the muscle group.
They can cause tenderness in the region and the spinous process or the bony tip extending from the lamina or part that can be felt when touching the back.
The pain is often described as burning.
Rhomboid Trigger Symptoms
A common symptom is superficial aching between the shoulder blades that individuals try to rub with their fingers to get relief.
Intense pain can extend upward to the shoulder area above the blade and into the neck area.
Individuals may hear or feel a crunching and snapping as they move the shoulder blades.
The common rounded-shoulder and forward-head hunching posture are nearly always present in individuals with these trigger points.
Middle Trapezius Trigger Points
The trapezius is the large, diamond-shaped muscle group that forms the base of the neck and upper back.
It has attachment points at the bottom of the skull, along the spine, collarbone, and shoulder blade.
When this muscle contracts, it moves the shoulder blade.
Movements can also affect the neck and head region.
Trigger points in the middle portion of this muscle refer to pain between the shoulder blades and the spine.
Trigger points develop for several reasons, including unhealthy postures, stress, injuries, falls, and sleeping positions.
Additionally, tension and added trigger points in the chest muscles can overload the Trapezius muscle fibers, causing trigger point development.
Trapezius Symptoms
It can be difficult to distinguish pain from the middle trapezius and rhomboid trigger points.
Pain in the middle trapezius can have more of a burning sensation and often extends over the thoracic spine.
The pain referral to the spine can activate secondary trigger points in the surrounding muscles.
Pectoralis Major Trigger Points
The Pectoralis Major muscle group is the large, flat muscles in the upper chest region.
The muscle has four overlapping sections that attach to the ribs, collarbone, chest bone, and upper arm at the shoulder.
The muscle group contracts when pushing with the arms in front of the body and rotating the arms inward towards the trunk.
Trigger points can radiate pain symptoms to the chest, shoulder, and breast regions.
Numbness and/or pain can radiate down the inside of the arm and into the fingers.
Trigger points in this muscle group can activate triggers in the upper back, causing pain symptoms between the shoulder blades.
Pectoralis Major Symptoms
Individuals will present with chest pain, front shoulder pain, and pain traveling down the inside of the arm to the elbow.
If referred pain occurs on the person’s left side, it can be similar to cardiac pain.
Consult a cardiologist to rule out cardiac involvement before investigating trigger points.
The pain will initially occur on one side of the chest but can spread to the other as it intensifies.
In many, the pain is only experienced with the movement of the arms and goes away or decreases with rest.
Simultaneous pain in the mid-back, between the shoulder blades, frequently occurs.
In women, there may be nipple sensitivity and pain in the breast.
The breast can become enlarged from the tension causing impaired lymphatic drainage.
Chiropractic Treatment
Chiropractors treat myofascial pain syndromes such as myofascial trigger points or adhesions with various therapies. A chiropractor will locate trigger points by pressing muscle tissue or manipulating the muscle fibers. Once the trigger points have been found, treatment can include:
Barbero, Marco, et al. “Myofascial pain syndrome and trigger points: evaluation and treatment in patients with musculoskeletal pain.” Current Opinion in Supportive and palliative care vol. 13,3 (2019): 270-276. doi:10.1097/SPC.0000000000000445
Bethers, Amber H et al. “Positional release therapy and therapeutic massage reduce muscle trigger and tender points.” Journal of Bodywork and movement therapies vol. 28 (2021): 264-270. doi:10.1016/j.jbmt.2021.07.005
Birinci, Tansu, et al. “Stretching exercises combined with ischemic compression in pectoralis minor muscle with latent trigger points: A single-blind, randomized, controlled pilot trial.” Complementary therapies in clinical practice vol. 38 (2020): 101080. doi:10.1016/j.ctcp.2019.101080
Farrell C, Kiel J. Anatomy, Back, Rhomboid Muscles. [Updated 2023 May 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK534856/
Gupta, Lokesh, and Shri Prakash Singh. “Ultrasound-Guided Trigger Point Injection for Myofascial Trigger Points in the Subscapularis and Pectoralis Muscles.” Yonsei medical journal vol. 57,2 (2016): 538. doi:10.3349/ymj.2016.57.2.538
Moraska, Albert F et al. “Responsiveness of Myofascial Trigger Points to Single and Multiple Trigger Point Release Massages: A Randomized, Placebo-Controlled Trial.” American Journal of physical medicine & Rehabilitation vol. 96,9 (2017): 639-645. doi:10.1097/PHM.0000000000000728
Sadria, Golnaz, et al. “A comparison of the effect of the active release and muscle energy techniques on the latent trigger points of the upper trapezius.” Journal of bodywork and movement therapies vol. 21,4 (2017): 920-925. doi:10.1016/j.jbmt.2016.10.005
Tiric-Campara, Merita, et al. “Occupational overuse syndrome (technological diseases): carpal tunnel syndrome, a mouse shoulder, cervical pain syndrome.” Acta informatica medica : AIM : journal of the Society for Medical Informatics of Bosnia & Herzegovina : casopis Drustva za medicinsku informatiku BiH vol. 22,5 (2014): 333-40. doi:10.5455/aim.2014.22.333-340
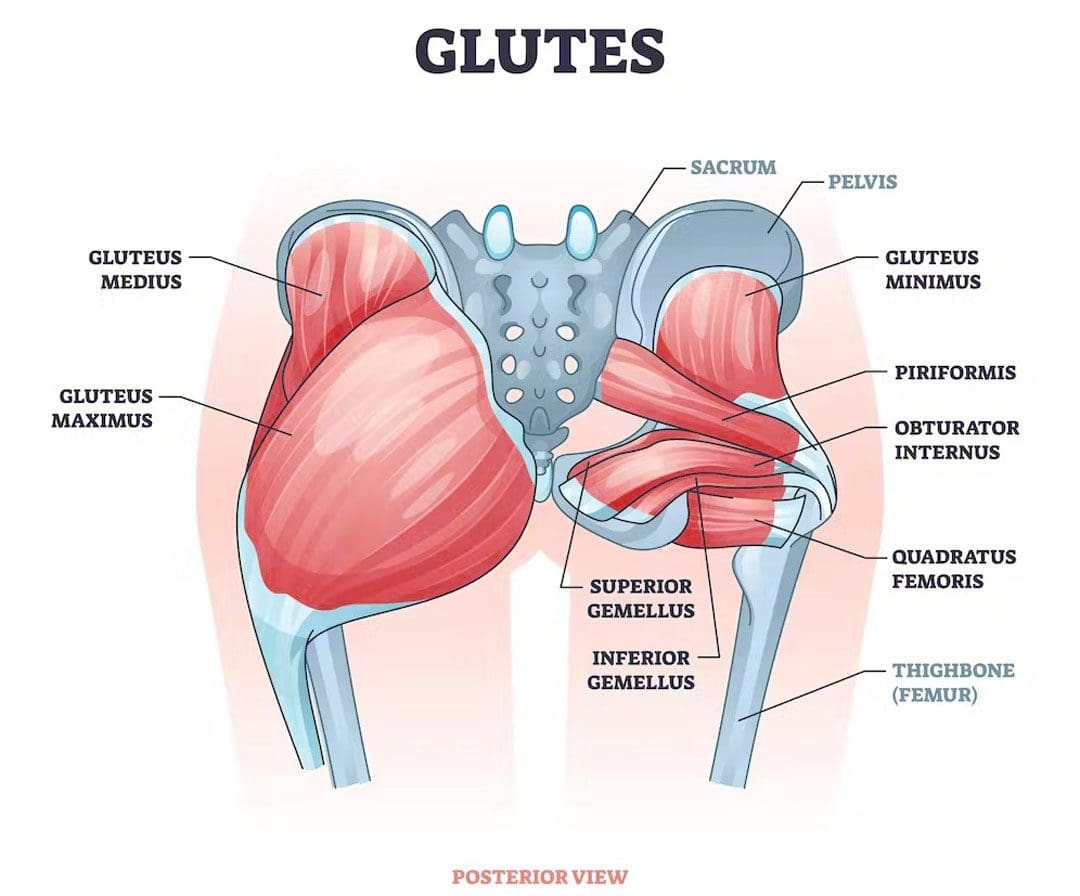
The gluteal muscles/glutes comprise the buttocks. They are a powerful muscle group that consists of three muscles. The gluteus maximus, gluteus medius, and gluteus minimus. The glute muscles help power physical performance and daily movements like walking, standing, and sitting and help to prevent injuries to the core, back, abdominal muscles, and other supporting muscles and tissues. Individuals can develop a glute imbalance where one side becomes more dominant and activates more or is higher than the other. An imbalance that is not addressed can lead to further muscle imbalance, posture problems, and pain issues. Injury Medical Chiropractic and Functional Medicine Clinic can develop a personalized treatment plan to relieve symptoms and restore alignment, balance, and health.
Glute Muscle Imbalance
Strong, healthy glutes promote lumbopelvic stability and rhythm, meaning they keep the low back and pelvis in correct alignment to prevent strains and injuries. Glute imbalance occurs when one side of the glutes is larger, stronger, or more dominant. Glute imbalances are common and part of normal human anatomy, as the body is not perfectly symmetrical. Shifting and utilizing the more dominant side when taking on weight or picking up objects is normal, so the one side gets bigger. Just as an individual prefers one hand, arm, and leg over another, one glute side can work harder and become stronger.
Causes
There are several causes of glute muscle imbalance, including:
Anatomical variations- Everyone has uniquely shaped muscles, attachment points, and nerve pathways. These variations can make one side of the glutes more dominant or stronger.
Unhealthy posture.
Back pain symptoms can cause individuals to take on unhealthy postures and positioning, like leaning on one side.
Pre-existing injuries.
Inadequate rehabilitation from a previous injury.
Nerve injuries.
Ankle sprains can lead to reduced glute activation.
Improper training
Leg length discrepancies
Atrophy
Spine condition
Job occupation
Sports factors may prioritize one side of the body over the other.
Shifting the Body
When pain presents in one body area, signals are sent to caution the other muscles to contract/tighten as a protective mechanism to prevent further injury. These changes alter movement patterns, leading to muscular imbalances in the glutes and other areas. Individuals who do not rehabilitate from an injury properly can be left with an imbalance.
Chiropractic Relief and Restoration
This condition needs to be addressed to prevent further injuries and issues with posture. Treatment varies depending on the individual and the extent of the problem. A treatment plan to prevent and improve some forms of glute imbalance may include the following.
Spinal decompression will stretch out the body and muscles to a workable position.
Therapeutic massage will relax the muscles and increase blood flow.
Chiropractic adjustments to realign the spine and body.
Targeted stretches and exercises will be provided to maintain alignment.
Unilateral training or training one side of the body at a time can help build and strengthen the weaker side.
Core strengthening can work out the differences on both sides of the body.
Chiropractic Approach for Pain Relief
References
Bini, Rodrigo Rico, and Alice Flores Bini. “Comparison of linea alba length and core-muscles engagement during core and lower back orientated exercises.” Journal of Bodywork and movement therapies vol. 28 (2021): 131-137. doi:10.1016/j.jbmt.2021.07.006
Buckthorpe, Matthew, et al. “ASSESSING AND TREATING GLUTEUS MAXIMUS WEAKNESS – A CLINICAL COMMENTARY.” International Journal of sports physical therapy vol. 14,4 (2019): 655-669.
Elzanie A, Borger J. Anatomy, Bony Pelvis and Lower Limb, Gluteus Maximus Muscle. [Updated 2023 Apr 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK538193/
Liu R, Wen X, Tong Z, Wang K, Wang C. Changes of gluteus medius muscle in the adult patients with unilateral developmental hip dysplasia. BMC Musculoskelet Disord. 2012;13(1):101. doi:10.1186/1471-2474-13-101
Lin CI, Khajooei M, Engel T, et al. The effect of chronic ankle instability on muscle activations in lower extremities. Li Y, ed. PLoS ONE. 2021;16(2):e0247581. doi:10.1371/journal.pone.0247581
Pool-Goudzwaard, A. L. et al. “Insufficient lumbopelvic stability: a clinical, anatomical and biomechanical approach to ‘a-specific’ low back pain.” Manual therapy vol. 3,1 (1998): 12-20. doi:10.1054/math.1998.0311
Vazirian, Milad, et al. “Lumbopelvic rhythm during trunk motion in the sagittal plane: A review of the kinematic measurement methods and characterization approaches.” Physical Therapy and Rehabilitation vol. 3 (2016): 5. doi:10.7243/2055-2386-3-5
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine