Back Clinic Injury Care Chiropractic and Physical Therapy Team. There are two approaches to injury care. They are active and passive treatment. While both can help get patients on the road toward recovery, only active treatment has a long-term impact and keeps patients moving.
We focus on treating injuries sustained in auto accidents, personal injuries, work injuries, and sports injuries and provide complete interventional pain management services and therapeutic programs. Everything from bumps and bruises to torn ligaments and back pain.
Passive Injury Care
A doctor or a physical therapist usually gives passive injury care. It includes:
Acupuncture
Applying heat/ice to sore muscles
Pain medication
It’s a good starting point to help reduce pain, but passive injury care isn’t the most effective treatment. While it helps an injured person feel better in the moment, the relief doesn’t last. A patient won’t fully recover from injury unless they actively work to return to their normal life.
Active Injury Care
Active treatment also provided by a physician or physical therapist relies on the injured person’s commitment to work. When patients take ownership of their health, the active injury care process becomes more meaningful and productive. A modified activity plan will help an injured person transition to full function and improve their overall physical and emotional wellness.
Spine, neck, and back
Headaches
Knees, shoulders, and wrists
Torn ligaments
Soft tissue injuries (muscle strains and sprains)
What does active injury care involve?
An active treatment plan keeps the body as strong and flexible as possible through a personalized work/transitional plan, which limits long-term impact and helps injured patients work toward a faster recovery. For example, in injury Medical & Chiropractic clinic’s injury care, a clinician will work with the patient to understand the cause of injury, then create a rehabilitation plan that keeps the patient active and brings them back to proper health in no time.
For answers to any questions, you may have, please call Dr. Jimenez at 915-850-0900
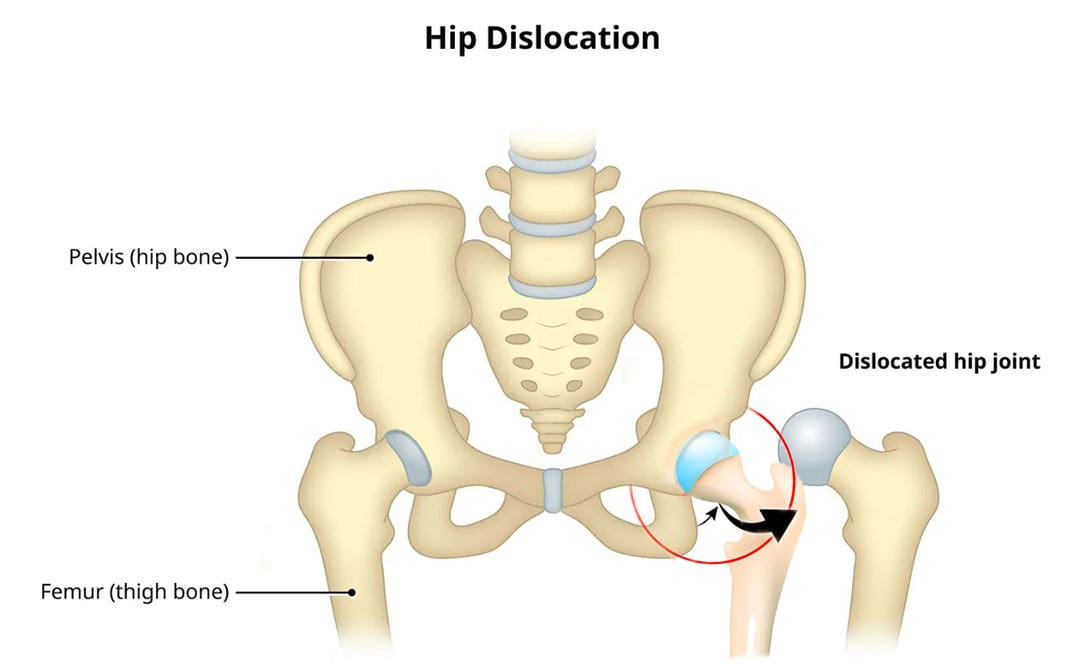
Can knowing treatment options for a dislocated hip help individuals expedite rehabilitation and recovery?
Dislocated Hip
A dislocated hip is an uncommon injury but can happen due to trauma or following hip replacement surgery. It usually occurs after severe trauma, including motor vehicle collisions, falls, and sometimes sports injuries. (Caylyne Arnold et al., 2017) A dislocated hip can also occur after hip replacement surgery. Other injuries like ligament tears, cartilage damage, and bone fractures can occur alongside the dislocation. Most hip dislocations are treated with a joint reduction procedure that resets the ball into the socket. It is usually done with sedation or general anesthesia. Rehabilitation takes time and could be a few months before full recovery. Physical therapy can help restore motion and strength in the hip.
What Is It?
If the hip is only partially dislocated, it’s called a hip subluxation. When this happens, the hip joint head only partially emerges from the socket. A dislocated hip is when the head or ball of the joint shifts or pops out of the socket. Because an artificial hip differs from a normal hip joint, the risk of dislocation increases after joint replacement. A study found that around 2% of individuals who undergo total hip replacement will experience hip dislocation within a year, with the cumulative risk increasing by approximately 1% over five years. (Jens Dargel et al., 2014) However, new technological prosthetics and surgical techniques are making this less common.
Hip Anatomy
The hip ball-and-socket joint is called the femoroacetabular joint.
The socket is called the acetabulum.
The ball is called the femoral head.
The bony anatomy and strong ligaments, muscles, and tendons help to create a stable joint. Significant force must be applied to the joint for a hip dislocation to occur. Some individuals report feeling a snapping sensation of the hip. This usually is not a hip dislocation but indicates a different disorder known as snapping hip syndrome. (Paul Walker et al., 2021)
Posterior Hip Dislocation
Around 90% of hip dislocations are posterior.
In this type, the ball is pushed backward from the socket.
A hip dislocation increases the risk of developing joint arthritis following the injury and can raise the risk of needing a hip replacement later in life. (Hsuan-Hsiao Ma et al., 2020)
Developmental Dislocation of the Hip
Some children are born with developmental dislocation of the hip or DDH.
Children with DDH have hip joints that did not form correctly during development.
This causes a loose fit in the socket.
In some cases, the hip joint is completely dislocated.
Joint reduction is the most common way to treat a dislocated hip. The procedure repositions the ball back into the socket and is usually done with sedation or under general anesthesia. Repositioning a hip requires significant force. A hip dislocation is considered an emergency, and reduction should be performed immediately after the dislocation to prevent permanent complications and invasive treatment. (Caylyne Arnold et al., 2017)
Once the ball is back in the socket, the healthcare provider will look for bone, cartilage, and ligament injuries.
Depending on what the healthcare provider finds, further treatment may be necessary.
Fractured or broken bones may need to be repaired to keep the ball within the socket.
Damaged cartilage may have to be removed.
Surgery
Surgery could be necessary to return the joint to its normal position. Hip arthroscopy can minimize the invasiveness of certain procedures. A surgeon inserts a microscopic camera into the hip joint to help the surgeon repair the injury using instruments inserted through other small incisions.
Hip replacement surgery replaces the ball and socket, a common and successful orthopedic surgical procedure. This surgery may be performed for various reasons, including trauma or arthritis, as it is common to develop early arthritis of the hip after this type of trauma. This is why many who have a dislocation ultimately need hip replacement surgery. As a major surgical procedure, it is not without risks. Possible complications include:
Infection
Aseptic loosening (the loosening of the joint without infection)
Hip dislocation
Recovery
Recovering from a hip dislocation is a long process. Individuals will need to walk with crutches or other devices early in recovery. Physical therapy will improve the range of motion and strengthen the muscles around the hip. Recovery time will depend on whether other injuries, such as fractures or tears, are present. If the hip joint was reduced and there were no other injuries, it may take six to ten weeks to recover to the point where weight can be placed on the leg. It could be between two and three months for a full recovery. Keeping weight off the leg is important until the surgeon or physical therapist gives the all-clear. Injury Medical Chiropractic and Functional Medicine Clinic will work with an individual’s primary healthcare provider and other surgeons or specialists to develop an optimal personalized treatment plan.
Chiropractic Solutions for Osteoarthritis
References
Arnold, C., Fayos, Z., Bruner, D., Arnold, D., Gupta, N., & Nusbaum, J. (2017). Managing dislocations of the hip, knee, and ankle in the emergency department [digest]. Emergency medicine practice, 19(12 Suppl Points & Pearls), 1–2.
Dargel, J., Oppermann, J., Brüggemann, G. P., & Eysel, P. (2014). Dislocation following total hip replacement. Deutsches Arzteblatt international, 111(51-52), 884–890. doi.org/10.3238/arztebl.2014.0884
Walker, P., Ellis, E., Scofield, J., Kongchum, T., Sherman, W. F., & Kaye, A. D. (2021). Snapping Hip Syndrome: A Comprehensive Update. Orthopedic reviews, 13(2), 25088. doi.org/10.52965/001c.25088
Cornwall, R., & Radomisli, T. E. (2000). Nerve injury in traumatic dislocation of the hip. Clinical orthopaedics and related research, (377), 84–91. doi.org/10.1097/00003086-200008000-00012
Kellam, P., & Ostrum, R. F. (2016). Systematic Review and Meta-Analysis of Avascular Necrosis and Posttraumatic Arthritis After Traumatic Hip Dislocation. Journal of orthopaedic trauma, 30(1), 10–16. doi.org/10.1097/BOT.0000000000000419
Ma, H. H., Huang, C. C., Pai, F. Y., Chang, M. C., Chen, W. M., & Huang, T. F. (2020). Long-term results in the patients with traumatic hip fracture-dislocation: Important prognostic factors. Journal of the Chinese Medical Association : JCMA, 83(7), 686–689. doi.org/10.1097/JCMA.0000000000000366
For individuals who lift weights, are there ways to protect the wrists and prevent injuries when lifting weights?
Wrist Protection
The wrists are complex joints. The wrists significantly contribute to stability and mobility when performing tasks or lifting weights. They provide mobility for movements using the hands and stability to carry and lift objects securely and safely (National Library of Medicine, 2024). Lifting weights is commonly performed to strengthen and stabilize the wrists; however, these movements can cause wrist pain and lead to injuries if not performed correctly. Wrist protection can keep wrists strong and healthy and is key to avoiding strains and injuries.
Wrist Strength
The wrist joints are set between the hand and forearm bones. Wrists are aligned in two rows of eight or nine total small bones/carpal bones and are connected to the arm and hand bones by ligaments, while tendons connect the surrounding muscles to the bones. Wrist joints are condyloid or modified ball and socket joints that assist with flexion, extension, abduction, and adduction movements. (National Library of Medicine. 2024) This means the wrists can move in all planes of motion:
Side to side
Up and down
Rotate
This provides a wide range of motion but can also cause excessive wear and tear and increase the risk of strain and injury. The muscles in the forearm and hand control finger movement necessary for gripping. These muscles and the tendons and ligaments involved run through the wrist. Strengthening the wrists will keep them mobile, help prevent injuries, and increase and maintain grip strength. In a review on weightlifters and powerlifters that examined the types of injuries they sustain, wrist injuries were common, with muscle and tendon injuries being the most common among weightlifters. (Ulrika Aasa et al., 2017)
Protecting the Wrists
Wrist protection can use a multi-approach, which includes consistently increasing strength, mobility, and flexibility to improve health and prevent injuries. Before lifting or engaging in any new exercise, individuals should consult their primary healthcare provider, physical therapist, trainer, medical specialist, or sports chiropractor to see which exercises are safe and provide benefits based on injury history and current level of health.
Increase Mobility
Mobility allows the wrists to have a full range of motion while retaining the stability necessary for strength and durability. Lack of mobility in the wrist joint can cause stiffness and pain. Flexibility is connected to mobility, but being overly flexible and lacking stability can lead to injuries. To increase wrist mobility, perform exercises at least two to three times a week to improve range of motion with control and stability. Also, taking regular breaks throughout the day to rotate and circle the wrists and gently pull back on the fingers to stretch them will help relieve tension and stiffness that can cause mobility problems.
Warm-Up
Before working out, warm up the wrists and the rest of the body before working out. Start with light cardiovascular to get the synovial fluid in the joints circulating to lubricate the joints, allowing for smoother movement. For example, individuals can make fists, rotate their wrists, perform mobility exercises, flex and extend the wrists, and use one hand to pull back the fingers gently. Around 25% of sports injuries involve the hand or wrist. These include hyperextension injury, ligament tears, front-inside or thumb-side wrist pain from overuse injuries, extensor injuries, and others. (Daniel M. Avery 3rd et al., 2016)
Strengthening Exercises
Strong wrists are more stable, and strengthening them can provide wrist protection. Exercises that improve wrist strength include pull-ups, deadlifts, loaded carries, and Zottman curls. Grip strength is vital for performing daily tasks, healthy aging, and continued success with weightlifting. (Richard W. Bohannon 2019) For example, individuals who have difficulty increasing the weight on their deadlifts because the bar slips from their hands could have insufficient wrist and grip strength.
Wraps
Wrist wraps or grip-assisting products are worth considering for those with wrist issues or concerns. They can provide added external stability while lifting, reducing grip fatigue and strain on the ligaments and tendons. However, it is recommended not to rely on wraps as a cure-all measure and to focus on improving individual strength, mobility, and stability. A study on athletes with wrist injuries revealed that the injuries still occurred despite wraps being worn 34% of the time prior to the injury. Because most injured athletes did not use wraps, this pointed to potential preventative measures, but the experts agreed more research is needed. (Amr Tawfik et al., 2021)
Preventing Overuse Injuries
When an area of the body undergoes too many repetitive motions without proper rest, it becomes worn, strained, or inflamed faster, causing overuse injury. The reasons for overuse injuries are varied but include not varying workouts enough to rest the muscles and prevent strain. A research review on the prevalence of injuries in weightlifters found that 25% were due to overuse tendon injuries. (Ulrika Aasa et al., 2017) Preventing overuse can help avoid potential wrist problems.
Proper Form
Knowing how to perform movements correctly and using proper form during each workout/training session is essential for preventing injuries. A personal trainer, sports physiotherapist, or physical therapist can teach how to adjust grip or maintain correct form.
Be sure to see your provider for clearance before lifting or starting an exercise program. Injury Medical Chiropractic and Functional Medicine Clinic can advise on training and prehabilitation or make a referral if one is needed.
Aasa, U., Svartholm, I., Andersson, F., & Berglund, L. (2017). Injuries among weightlifters and powerlifters: a systematic review. British journal of sports medicine, 51(4), 211–219. doi.org/10.1136/bjsports-2016-096037
Avery, D. M., 3rd, Rodner, C. M., & Edgar, C. M. (2016). Sports-related wrist and hand injuries: a review. Journal of orthopaedic surgery and research, 11(1), 99. doi.org/10.1186/s13018-016-0432-8
Bohannon R. W. (2019). Grip Strength: An Indispensable Biomarker For Older Adults. Clinical interventions in aging, 14, 1681–1691. doi.org/10.2147/CIA.S194543
Tawfik, A., Katt, B. M., Sirch, F., Simon, M. E., Padua, F., Fletcher, D., Beredjiklian, P., & Nakashian, M. (2021). A Study on the Incidence of Hand or Wrist Injuries in CrossFit Athletes. Cureus, 13(3), e13818. doi.org/10.7759/cureus.13818
For athletes and sports enthusiasts, a torn triceps can be a serious injury. Can knowing their symptoms, causes, risk factors, and potential complications help healthcare providers develop an effective treatment plan?
Torn Triceps Injury
The triceps is the muscle on the back of the upper arm that allows the elbow to straighten. Fortunately, triceps tears are uncommon, but they can be serious. The injury affects men more often than women and usually occurs from trauma, sports, and/or exercise activities. Depending on the extent and severity of the injury, a torn triceps injury can require splinting, physical therapy, and possibly surgery to regain movement and strength. Recovery after a triceps tear typically lasts around six months. (The Ohio State University Wexner Medical Center. 2021)
Anatomy
The triceps brachii muscle, or triceps, runs along the back of the upper arm. It is named tri- because it has three heads – the long, medial, and lateral head. (Sendic G. 2023) The triceps originates at the shoulder and attaches to the shoulder blade/scapula and upper arm bone/humerus. At the bottom, it attaches to the point of the elbow. This is the bone on the pinky side of the forearm, known as the ulna. The triceps cause movement at the shoulder and the elbow joint. At the shoulder, it performs extension or backward movement of the arm and adduction or moving the arm toward the body. The main function of this muscle is at the elbow, where it performs extension or straightening of the elbow. The triceps work the opposite of the biceps muscle on the front of the upper arm, which conducts flexion or bending of the elbow.
Triceps Tear
Tears can occur anywhere along the length of a muscle or tendon, which is the structure that attaches the muscle to the bones. Triceps tears commonly occur in the tendon connecting the triceps to the back of the elbow. Muscle and tendon tears are graded from 1 to 3 based on severity. (Alberto Grassi et al., 2016)
Grade 1 Mild
These small tears cause pain that worsens with movement.
There is some swelling, bruising, and minimal loss of function.
Grade 2 Moderate
These tears are larger and have moderate swelling and bruising.
The fibers are partially torn and stretched.
Up to 50% loss of function.
Grade 3 Severe
This is the worst type of tear, where the muscle or tendon is completely torn.
These injuries cause severe pain and disability.
Symptoms
Triceps tears cause immediate pain in the back of the elbow and upper arm that worsens when trying to move the elbow. Individuals might also feel and/or hear a popping or tearing sensation. There will be swelling, and the skin will likely be red and/or bruised. With a partial tear, the arm will feel weak. If there is a complete tear, there will be significant weakness when straightening the elbow. Individuals may also notice a lump on the back of their arm where the muscles have contracted and knotted together.
Causes
Triceps tears usually occur during trauma, when the muscle is contracted and an external force pushes the elbow into a bent position. (Kyle Casadei et al., 2020) One of the most common causes is by falling on an outstretched arm. Triceps tears also occur during sports activities like:
Throwing a baseball
Blocking in a football game
Gymnastics
Boxing
When a player falls and lands on their arm.
Tears can also happen when using heavy weights during triceps-targeted exercises, such as the bench press.
Tears can also occur from direct trauma to the muscle, like a motor vehicle accident, but are less common.
Long-Term
Triceps tears can develop over time as a result of tendonitis. This condition usually occurs from repetitive use of the triceps muscle during activities like manual labor or exercise. Triceps tendonitis is sometimes referred to as weightlifter’s elbow. (Orthopedic & Spine Center. N.D.) The strain on tendons causes tiny tears that the body typically heals. However, if more strain is placed on the tendon than it can keep up with, the tiny tears can begin to grow.
Risk Factors
Risk factors can increase the risk of a triceps tear. Underlying medical conditions can weaken tendons, increasing the risk of injury, and can include: (Tony Mangano et al., 2015)
Diabetes
Rheumatoid arthritis
Hyperparathyroidism
Lupus
Xanthoma – fatty deposits of cholesterol under the skin.
Hemangioendothelioma – cancerous or noncancerous tumors caused by abnormal growth of blood vessel cells.
Chronic kidney failure
Chronic tendonitis or bursitis in the elbow.
Individuals who have had cortisone shots in the tendon.
Individuals using anabolic steroids.
Triceps tears tend to occur more commonly in males between 30 and 50. (Ortho Bullets. 2022) This comes from participating in activities like football, weightlifting, bodybuilding, and manual labor, which also increases the risk of injury.
Treatment
Treatment depends on which part of the triceps is affected and the extent of the damage. It may only need resting for a few weeks, physical therapy, or require surgery.
Nonsurgical
Partial tears in the triceps that involve less than 50% of the tendon can often be treated without surgery. (Mehmet Demirhan, Ali Ersen 2016) Initial treatment includes:
Splinting the elbow with a slight bend for four to six weeks allows the injured tissue to heal. (Ortho Bullets. 2022)
During this time, ice can be applied to the area for 15 to 20 minutes several times daily to help decrease pain and swelling.
Non-steroidal anti-inflammatory medications/NSAIDs – Aleve, Advil, and Bayer can help reduce inflammation.
Other over-the-counter medications like Tylenol can help decrease the pain.
Once the splint is removed, physical therapy will help restore movement and strength in the elbow.
Full movement is expected to return within 12 weeks, but full strength will not return until six to nine months after the injury. (Mehmet Demirhan, Ali Ersen 2016)
Surgery
Triceps tendon tears that involve more than 50% of the tendon require surgery. In some cases, however, surgery may still be recommended for tears smaller than 50% if the individual has a physically demanding job or plans to resume playing sports at a high level. Tears in the muscle belly or area where the muscle and tendon join are typically sewn back together. If the tendon is no longer attached to the bone, it is screwed back on. Recovery and physical therapy after surgery depend on the specific surgeon’s protocols. In general, individuals will spend a couple of weeks in a brace. Around four weeks after surgery, individuals will be able to start moving the elbow again. However, they won’t be able to start doing heavy lifting for four to six months. (Ortho Bullets. 2022) (Mehmet Demirhan, Ali Ersen 2016)
Complications
Complications can occur after triceps repair, whether there was surgery or not. For example, individuals may have problems regaining full elbow extension or straightening. They are also at a higher risk of re-rupture if they try to use the arm before it’s fully healed. (Mehmet Demirhan, Ali Ersen 2016)
Grassi, A., Quaglia, A., Canata, G. L., & Zaffagnini, S. (2016). An update on the grading of muscle injuries: a narrative review from clinical to comprehensive systems. Joints, 4(1), 39–46. doi.org/10.11138/jts/2016.4.1.039
Casadei, K., Kiel, J., & Freidl, M. (2020). Triceps Tendon Injuries. Current sports medicine reports, 19(9), 367–372. doi.org/10.1249/JSR.0000000000000749
Mangano, T., Cerruti, P., Repetto, I., Trentini, R., Giovale, M., & Franchin, F. (2015). Chronic Tendonopathy as a Unique Cause of Non Traumatic Triceps Tendon Rupture in a (Risk Factors Free) Bodybuilder: A Case Report. Journal of orthopaedic case reports, 5(1), 58–61. doi.org/10.13107/jocr.2250-0685.257
Can physical therapy with instrument-assisted soft tissue mobilization or IASTM improve mobility, flexibility, and health for individuals with musculoskeletal injuries or illnesses?
Instrument Assisted Soft Tissue Mobilization
Instrument-assisted soft tissue mobilization or IASTM is also known as the Graston technique. It is a myofascial release and massage technique used in physical therapy where the therapist uses metal or plastic tools to improve soft tissue mobility in the body. The ergonomically shaped tool is gently or vigorously scraped and rubbed across the injured or painful area. The rubbing is used to locate and release tightness in the fascia/collagen covering the muscles and the tendons. This helps reduce pain and improve movement.
Individuals often develop tissue tightness or restrictions in the muscles and fascia after an injury. These soft tissue restrictions can limit the range of motion – ROM and can trigger pain symptoms. (Kim J, Sung DJ, Lee J. 2017)
History
The Graston technique of instrument-assisted soft tissue mobilization was developed by an athlete who created their instruments to treat soft tissue injuries. The practice has grown with input from medical experts, trainers, researchers, and clinicians.
Physical therapists use different types of tools to perform IASTM.
These massage instruments comprise various types for specific massage and release.
The Graston company designs some of the tools.
Other companies have their version of metal or plastic scraping and rubbing tools.
The objective is to help release soft tissue and myofascial restrictions to improve body movement. (Kim J, Sung DJ, Lee J. 2017)
How It Works
The theory is that scraping the tissues causes microtrauma to the affected area, activating the body’s natural inflammatory response. (Kim J, Sung DJ, Lee J. 2017)
The body activates to reabsorb the tightened or scar tissue, causing the restriction.
The therapist can then stretch the adhesions to alleviate pain and improve mobility.
Treatment
Certain conditions respond well to instrument-assisted soft tissue mobilization, including (Kim J, Sung DJ, Lee J. 2017)
Limited mobility
Decreased muscle recruitment
Loss of range of motion – ROM
Pain with movement
Excessive scar tissue formation
Augmented soft tissue mobilization or ASTM techniques can treat certain injuries and medical conditions that include:
A review compared hands-on myofascial release to instrument myofascial release for chronic low back pain. (Williams M. 2017)
Little difference was found between the two techniques for pain relief.
Another review compared IASTM to other methods for treating pain and function loss. (Matthew Lambert et al., 2017)
The researchers concluded that IASTM could positively affect blood circulation and tissue flexibility and reduce pain.
Another study examined the use of IASTM, pseudo-fake ultrasound therapy, and spinal manipulation for patients with thoracic/upper back pain. (Amy L. Crothers et al., 2016)
All groups improved over time with no significant negative events.
The researchers concluded that instrument-assisted soft tissue mobilization is no more or less effective than spinal manipulation or pseudo-ultrasound therapy for thoracic back pain.
Every case is different, and musculoskeletal conditions respond differently to various treatments. For any questions or concerns, contact your primary healthcare provider to determine if IASTM is an appropriate treatment that can help.
From Injury To Recovery
References
Kamali, F., Panahi, F., Ebrahimi, S., & Abbasi, L. (2014). Comparison between massage and routine physical therapy in women with sub acute and chronic nonspecific low back pain. Journal of back and musculoskeletal rehabilitation, 27(4), 475–480. doi.org/10.3233/BMR-140468
Kim, J., Sung, D. J., & Lee, J. (2017). Therapeutic effectiveness of instrument-assisted soft tissue mobilization for soft tissue injury: mechanisms and practical application. Journal of exercise rehabilitation, 13(1), 12–22. doi.org/10.12965/jer.1732824.412
Chughtai, M., Newman, J. M., Sultan, A. A., Samuel, L. T., Rabin, J., Khlopas, A., Bhave, A., & Mont, M. A. (2019). Astym® therapy: a systematic review. Annals of translational medicine, 7(4), 70. doi.org/10.21037/atm.2018.11.49
Matthew Lambert, Rebecca Hitchcock, Kelly Lavallee, Eric Hayford, Russ Morazzini, Amber Wallace, Dakota Conroy & Josh Cleland (2017) The effects of instrument-assisted soft tissue mobilization compared to other interventions on pain and function: a systematic review, Physical Therapy Reviews, 22:1-2, 76-85, DOI: 10.1080/10833196.2017.1304184
Crothers, A. L., French, S. D., Hebert, J. J., & Walker, B. F. (2016). Spinal manipulative therapy, Graston technique® and placebo for non-specific thoracic spine pain: a randomised controlled trial. Chiropractic & manual therapies, 24, 16. doi.org/10.1186/s12998-016-0096-9
For individuals dealing with knee pain symptoms from injury and/or arthritis, can incorporating an acupuncture and/or electroacupuncture treatment plan help in pain relief and management?
Acupuncture For Knee Pain
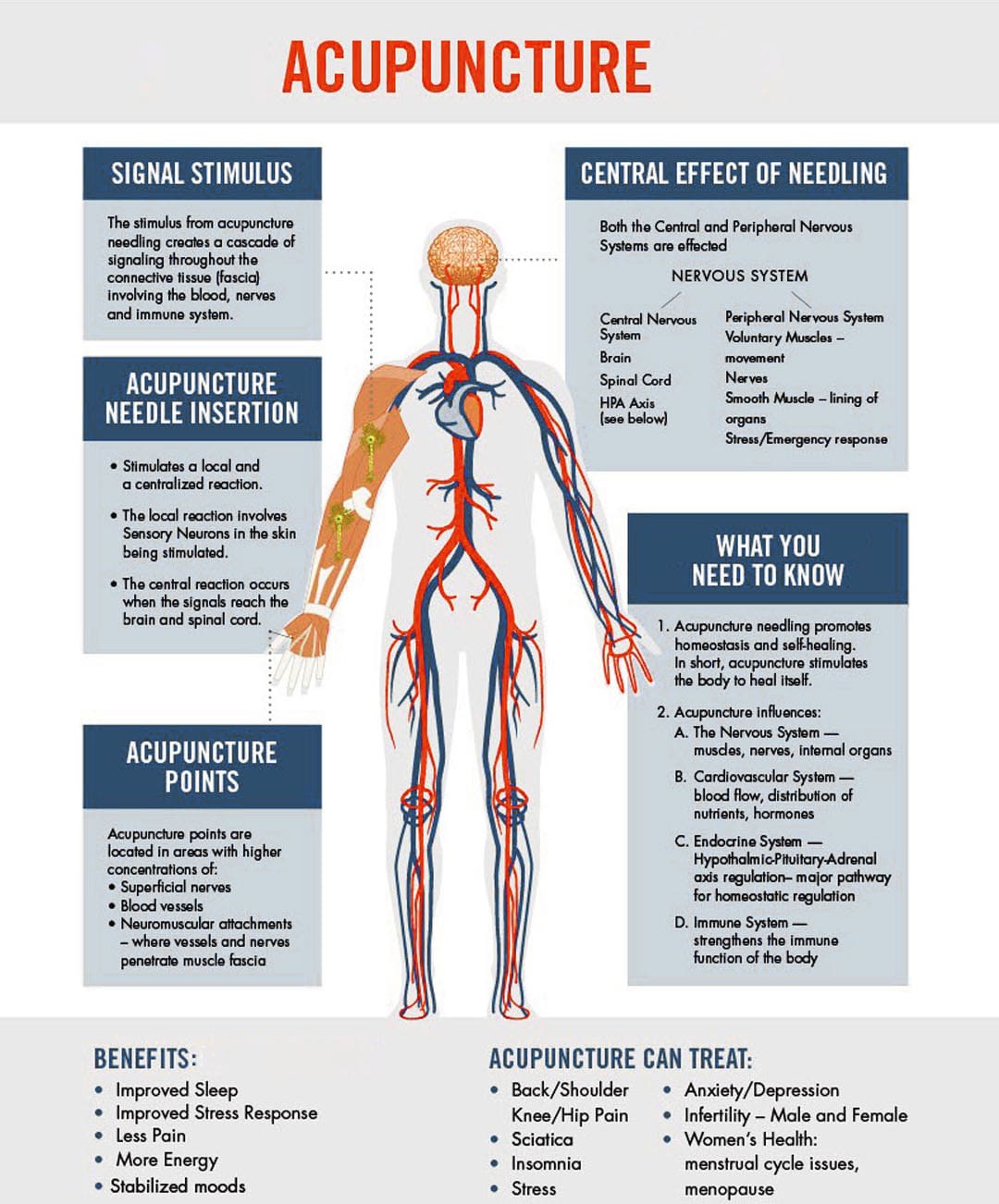
Acupuncture involves inserting very thin needles into the skin at specific acupoints on the body. It is based on the premise that the needles restore the flow of the body’s energy to activate and promote healing, relieve pain, and help the body relax.
Acupuncture can help address various health conditions, including knee pain caused by arthritis or injury.
Depending on the type and severity of pain, treatments can help reduce the pain for days or weeks.
Acupuncture is often used as a complementary therapy – treatment in addition to other treatment or therapy strategies like massage and chiropractic.
Acupuncture Benefits
Knee pain caused by osteoarthritis or injury can reduce flexibility, mobility, and quality of life. Acupuncture can help provide relief.
When the acupuncture needles are placed on the body, a signal is sent along the spinal cord to the brain, which triggers a release of endorphins/pain hormones. Medical researchers believe this helps reduce pain. (Qian-Qian Li et al., 2013) Acupuncture also helps decrease the production of cortisol, a hormone that helps control inflammation. (Qian-Qian Li et al., 2013) With reduced pain sensations and less inflammation after acupuncture treatments, knee function and mobility can be improved.
Various factors play a role in the pain relief experienced from acupuncture. Some evidence suggests that an individual’s expectations may impact the results of acupuncture treatment. (Stephanie L. Prady et al., 2015)
Researchers are currently assessing whether the expectation that acupuncture is beneficial contributes to a better outcome after treatment. (Zuoqin Yang et al., 2021)
In 2019, acupuncture was recommended in treating knee osteoarthritis in the American College of Rheumatology/Arthritis Foundation guidelines for hand, hip, and knee osteoarthritis pain management. (Sharon L. Kolasinski et al., 2020)
Research
Different clinical studies support acupuncture’s ability to help in knee pain relief and management.
One study found that acupuncture helps manage various conditions that cause chronic pain. (Andrew J. Vickers et al., 2012)
A scientific review analyzed previous studies on pain management interventions after knee surgery and found supporting evidence that the treatments delayed and reduced the use of medications for pain relief post-surgery. (Dario Tedesco et al., 2017)
Osteoarthritis
A systematic review analyzed randomized control studies to determine whether or not acupuncture reduced pain and improved joint function in individuals with chronic osteoarthritis knee pain. (Xianfeng Lin et al., 2016)
Individuals received six to twenty-three weekly acupuncture sessions for three to 36 weeks.
The analysis determined that acupuncture can improve short and long-term physical function and mobility and provide up to 13 weeks of pain relief in individuals with chronic knee pain caused by osteoarthritis.
Rheumatoid Arthritis
Rheumatoid arthritis is a chronic disease that affects joints, including the knee joint, causing pain and stiffness.
Acupuncture is beneficial in treating rheumatoid arthritis/RA.
A review found that acupuncture alone and in combination with other treatment modalities benefits individuals with RA. (Pei-Chi, Chou Heng-Yi Chu 2018)
Acupuncture is believed to have anti-inflammatory and antioxidant effects to help regulate immune system function.
Chronic Knee Pain
Various conditions and injuries can cause chronic knee pain, making mobility difficult.
Individuals with joint pain often turn to complementary therapies for pain relief management, with acupuncture being one of the popular modalities. (Michael Frass et al., 2012)
Working with a licensed, professional acupuncture practitioner can reduce the risk of unwanted side effects and complications.
Types
Other acupuncture options that may be offered include:
Electroacupuncture
A modified form of acupuncture where a mild electrical current passes through the needles, providing additional stimulation to the acupoints.
In one research study, individuals with knee osteoarthritis reported significant improvements in their pain, stiffness, and physical function after electroacupuncture treatment. (Ziyong Ju et al., 2015)
Auricular
Auricular or ear acupuncture works on acupoints in the ear corresponding to the body’s different parts.
A research review analyzed several studies on auricular acupuncture for pain relief and found that it can provide relief within 48 hours of pain onset. (M. Murakami et al., 2017)
Battlefield Acupuncture
The military and veteran healthcare facilities use a unique form of auricular acupuncture for pain management.
Studies show that it is effective at providing immediate pain relief, but more research is necessary to determine long-term pain relief effectiveness. (Anna Denee Montgomery, Ronovan Ottenbacher 2020)
Before trying acupuncture, consult a healthcare professional for guidance, as it may be integrated with other therapies and lifestyle adjustments.
Overcoming an ACL Injury
References
Li, Q. Q., Shi, G. X., Xu, Q., Wang, J., Liu, C. Z., & Wang, L. P. (2013). Acupuncture effect and central autonomic regulation. Evidence-based complementary and alternative medicine : eCAM, 2013, 267959. doi.org/10.1155/2013/267959
Prady, S. L., Burch, J., Vanderbloemen, L., Crouch, S., & MacPherson, H. (2015). Measuring expectations of benefit from treatment in acupuncture trials: a systematic review. Complementary therapies in medicine, 23(2), 185–199. doi.org/10.1016/j.ctim.2015.01.007
Yang, Z., Li, Y., Zou, Z., Zhao, Y., Zhang, W., Jiang, H., Hou, Y., Li, Y., & Zheng, Q. (2021). Does patient’s expectation benefit acupuncture treatment?: A protocol for systematic review and meta-analysis. Medicine, 100(1), e24178. doi.org/10.1097/MD.0000000000024178
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., Wise, B., … Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research, 72(2), 149–162. doi.org/10.1002/acr.24131
Vickers, A. J., Cronin, A. M., Maschino, A. C., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Witt, C. M., Linde, K., & Acupuncture Trialists’ Collaboration (2012). Acupuncture for chronic pain: individual patient data meta-analysis. Archives of internal medicine, 172(19), 1444–1453. doi.org/10.1001/archinternmed.2012.3654
Tedesco, D., Gori, D., Desai, K. R., Asch, S., Carroll, I. R., Curtin, C., McDonald, K. M., Fantini, M. P., & Hernandez-Boussard, T. (2017). Drug-Free Interventions to Reduce Pain or Opioid Consumption After Total Knee Arthroplasty: A Systematic Review and Meta-analysis. JAMA surgery, 152(10), e172872. doi.org/10.1001/jamasurg.2017.2872
Lin, X., Huang, K., Zhu, G., Huang, Z., Qin, A., & Fan, S. (2016). The Effects of Acupuncture on Chronic Knee Pain Due to Osteoarthritis: A Meta-Analysis. The Journal of bone and joint surgery. American volume, 98(18), 1578–1585. doi.org/10.2106/JBJS.15.00620
Chou, P. C., & Chu, H. Y. (2018). Clinical Efficacy of Acupuncture on Rheumatoid Arthritis and Associated Mechanisms: A Systemic Review. Evidence-based complementary and alternative medicine : eCAM, 2018, 8596918. doi.org/10.1155/2018/8596918
Frass, M., Strassl, R. P., Friehs, H., Müllner, M., Kundi, M., & Kaye, A. D. (2012). Use and acceptance of complementary and alternative medicine among the general population and medical personnel: a systematic review. Ochsner journal, 12(1), 45–56.
Hinman, R. S., McCrory, P., Pirotta, M., Relf, I., Forbes, A., Crossley, K. M., Williamson, E., Kyriakides, M., Novy, K., Metcalf, B. R., Harris, A., Reddy, P., Conaghan, P. G., & Bennell, K. L. (2014). Acupuncture for chronic knee pain: a randomized clinical trial. JAMA, 312(13), 1313–1322. doi.org/10.1001/jama.2014.12660
Ju, Z., Guo, X., Jiang, X., Wang, X., Liu, S., He, J., Cui, H., & Wang, K. (2015). Electroacupuncture with different current intensities to treat knee osteoarthritis: a single-blinded controlled study. International journal of clinical and experimental medicine, 8(10), 18981–18989.
Murakami, M., Fox, L., & Dijkers, M. P. (2017). Ear Acupuncture for Immediate Pain Relief-A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain medicine (Malden, Mass.), 18(3), 551–564. doi.org/10.1093/pm/pnw215
Montgomery, A. D., & Ottenbacher, R. (2020). Battlefield Acupuncture for Chronic Pain Management in Patients on Long-Term Opioid Therapy. Medical acupuncture, 32(1), 38–44. doi.org/10.1089/acu.2019.1382
Knee injuries can present in physically active individuals that lift weights. Can understanding the types of weightlifting knee injuries help in prevention?
Weightlifting Knee Injuries
Weight training is very safe for the knees as regular weight training can improve knee strength and prevent injury as long as the correct form is followed. For Individuals with knee injuries from other activities, incorrect weight-training exercises could worsen the injury. (Ulrika Aasa et al., 2017) As well as, sudden twisting movements, poor alignment, and pre-existing injuries can increase the risk of worsening or creating further injuries. (Hagen Hartmann et al, 2013) The body and the knees are designed to support vertical forces on the joints.
Common Injuries
Weightlifting knee injuries occur as the knee joints endure a wide range of stresses and strains. In weight training, the ligaments that attach to the complex bone system of the knee joint can be damaged by incorrect movements, overloading the weight, and increasing the weight too soon. These injuries can result in pain, swelling, and immobility that can range from minor to severe, from a sprain or a slight tear to a complete tear in serious cases.
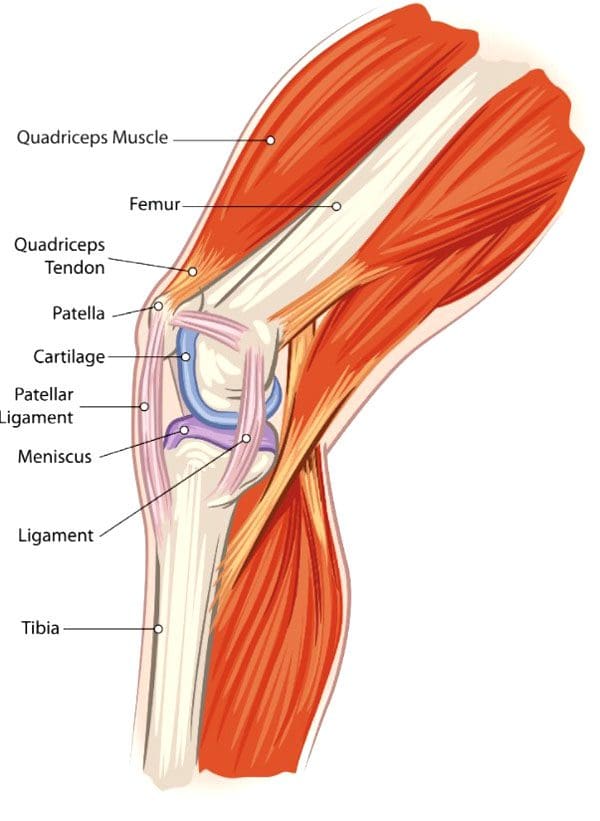
Anterior Cruciate Ligament – ACL – Injury
This ligament attaches the thigh’s femur bone to the lower leg’s shin bone/tibia and controls excessive rotation or extension of the knee joint. (American Academy of Family Physicians. 2024)
Anterior means front.
ACL injuries are seen mostly in athletes but can happen to anybody.
Severe damage to the ACL usually means surgical reconstruction and up to 12 months of rehabilitation.
When weightlifting, try to avoid twisting knee movements, intentionally or accidentally, under excessive load.
Posterior Cruciate Ligament – PCL – Injury
The PCL connects the femur and tibia at different points to the ACL.
It controls any backward motion of the tibia at the joint.
Injuries occur most with high-impact forces as a result of accidents and sometimes in activities where forceful trauma to the knee occurs.
Medial Collateral Ligament – MCL – Injury
This ligament maintains the knee from bending too far to the inside/medially.
Injuries mostly occur from impact to the outside of the knee or from accidental bodyweight force on the leg that bends at an unusual angle.
Lateral Collateral Ligament – LCL – Injury
This ligament connects the smaller bone of the lower leg/fibula to the femur.
It is opposite to the MCL.
It maintains excessive outward movement.
LCL injuries occur when a force pushes the knee out.
Cartilage Injury
Cartilage prevents bones from rubbing together and cushions impact forces.
Knee menisci are cartilage that cushions the knee joints inside and outside.
Other types of cartilage protect the thigh and shin bones.
When cartilage gets torn or damaged, surgery may be required.
Tendonitis
Aggravated and overused knee tendons can lead to weightlifting knee injuries.
A related injury known as iliotibial band syndrome/ITB causes pain to the outside of the knee, usually in runners, but it can occur from overuse.
Rest, stretching, physical therapy, and anti-inflammatory medication are a common treatment plan.
The condition causes the cartilage to deteriorate and bones to rub together, resulting in pain and stiffness.
Prevention
Individuals can minimize their risk of weightlifting knee injuries and pain by following their doctor’s and personal trainers’ recommendations.
Individuals with an existing knee injury should follow their doctor’s or physical therapist’s recommendations.
A knee sleeve can keep the muscles and joints secure, providing protection and support.
Stretching the leg and knee muscles can maintain joint flexibility.
Avoid sudden lateral movements.
Possible recommendations can include:
Avoiding Certain Exercises
Isolation exercises like leg curls, standing, or on a bench, as well as using the leg extension machine, can stress the knee.
Deep Squat Training
Research shows that the deep squat can protect against lower leg injury if the knee is healthy. However, this is when done with proper technique, under expert supervision, and with a gradual progressive load. (Hagen Hartmann et al, 2013)
Individuals should talk to their doctor before beginning a new exercise routine. A personal trainer can provide training in learning the proper technique and weightlifting form.
How I Tore my ACL Part 2
References
Aasa, U., Svartholm, I., Andersson, F., & Berglund, L. (2017). Injuries among weightlifters and powerlifters: a systematic review. British journal of sports medicine, 51(4), 211–219. doi.org/10.1136/bjsports-2016-096037
Hartmann, H., Wirth, K., & Klusemann, M. (2013). Analysis of the load on the knee joint and vertebral column with changes in squatting depth and weight load. Sports medicine (Auckland, N.Z.), 43(10), 993–1008. doi.org/10.1007/s40279-013-0073-6
Mellinger, S., & Neurohr, G. A. (2019). Evidence based treatment options for common knee injuries in runners. Annals of translational medicine, 7(Suppl 7), S249. doi.org/10.21037/atm.2019.04.08
Driban, J. B., Hootman, J. M., Sitler, M. R., Harris, K. P., & Cattano, N. M. (2017). Is Participation in Certain Sports Associated With Knee Osteoarthritis? A Systematic Review. Journal of athletic training, 52(6), 497–506. doi.org/10.4085/1062-6050-50.2.08
For individuals dealing with injuries and pain conditions, can incorporating acupuncture into a treatment plan help alleviate and manage pain?
Acupuncture Pain Management
Pain management techniques include physical therapy, medications, cold therapies, chiropractic, and massages. One method that is growing is acupuncture. (World Health Organization. 2021) According to a report by the World Health Organization, acupuncture is the most commonly used form of traditional medicine practiced globally. (World Health Organization. 2021) More than 10 million acupuncture treatments are administered annually in the U.S. (Jason Jishun Hao, Michele Mittelman. 2014)
What Is It?
Acupuncture is a medical practice that involves placing solid but super thin needles at specific points in the body to treat certain health issues. They can be used on their own or stimulated with electric currents, called electroacupuncture. Acupuncture originated in China about 3,000 years ago and is known as traditional Chinese medicine or TCM. In more recent years, the practice has gained acceptance and demand worldwide. (Jason Jishun Hao, Michele Mittelman. 2014)
How Does It Work?
Acupuncture pain management works by balancing the flow of qi/chi/energy, which moves through meridians, or channels in the body. By inserting needles into specific points along these channels, balance is reestablished for overall health and well-being. When the energy is imbalanced due to internal and external stressors that can include injuries, underlying conditions, unhealthy diet, and stress, individuals can present with symptoms and illness. Using diagnostic techniques and comprehensive interviews, practitioners can determine which organ systems and meridian channels need addressing to restore function. There are more than 2,000 acupoints in the body. (Johns Hopkins Medicine. 2024) Each point has its own purpose and function: some increase energy, others decrease it, helping balance the body to support healing and recovery. Acupuncture pain management goes beyond energy healing and can help alleviate pain by stimulating nerves, muscles, and fascia/connective tissue, regulating immune response, nervous system response, lymphatic flow, and increasing muscle relaxation.
Types
Different types of acupuncture have been modified in training and styles, but all involve needling into certain points and include:
Orthopedic/Dry Needling
This technique combines Traditional Chinese Medicine and structure manipulation to treat pain, tissue injuries, imbalances in the body, and other general systemic disorders.
Five Element Style
This is a spiritual and emotional technique that uses the five elements of nature, including wood, fire, earth, metal, and water, to transfer energy, creating balance in the body.
Japanese Style
uses similar techniques to TCM but uses a more subtle approach, such as using fewer needles or inserting them at lower depths in the body.
Korean
This technique uses both techniques from Chinese and Japanese acupuncture.
Practitioners may use more needles and different kinds of needles, like a copper variety, instead of the standard stainless steel type.
This type of acupuncture uses only acupoints on the hand to treat different areas of the body.
Auricular
This is similar to Korean acupuncture but relies on certain points in the ear to treat other areas of the body.
The goal is to overcome imbalances and disharmonies.
Distal
This technique treats pain indirectly.
Practitioners place needles in spots other than the area of discomfort.
For example, practitioners may place needles around the elbows for knee pain or the lower legs for shoulder pain.
Acupressure
This form of therapy stimulates different acupoints without using needles.
Practitioners use precise finger placements, hands, or other tools and essential oils to apply pressure over specific points to enhance energy flow.
Providers can combine and use various forms based on an individual’s needs.
Conditions
One analysis of more than 2,000 scientific reviews of acupuncture therapies found it to be effective for post-stroke aphasia, neck, shoulder, lower back pain, muscle pain, fibromyalgia pain, lactation issues after delivery, vascular dementia symptoms, and allergy symptoms. (Liming Lu et al., 2022) A study on mice by neuroscientists found that electroacupuncture can decrease inflammation. (Shenbin Liu et al., 2020) The National Center for Complementary and Integrative Health found that acupuncture can be helpful for: (National Center for Complementary and Integrative Health. 2022)
Nausea and vomiting in cancer patients undergoing treatment
Chronic prostatitis
Digestion
Irritable bowel syndrome
Seasonal allergies
Urinary incontinence
Infertility
Asthma
Quitting smoking
Depression
Safety
When the treatment is performed by a highly trained, licensed, and certified acupuncturist, it is very safe. The most common serious adverse events were pneumothorax/collapsed lung, cardiovascular problems, and fainting, which in some cases caused trauma, like fractures. (Petra Bäumler et al., 2021) There are some short-term risks associated with acupuncture, including:
Pain
Bleeding
Bruising
Drowsiness
Dizziness for individuals that have not eaten or fear of needles.
Serious side effects associated with acupuncture, like a punctured lung or infection, are very rare. For individuals that have a metal allergy, infection, or open wound in the area where the needles will be inserted, it is recommended to avoid acupuncture. Individuals who have a bleeding disorder, are taking any medicines like an anticoagulant, or are pregnant, should talk to the acupuncturist before beginning a treatment plan.
What to Expect
Everyone’s visit will be tailored to their specific needs, and the first visit will likely last an hour or two. The initial evaluation will include a full medical/health history. The individual will spend a few minutes discussing concerns and health goals with the acupuncturist. Individuals will be asked to lie on the treatment table so the practitioner can access their limbs, back, and abdomen. After inserting needles, they will stay in place for about 20 to 30 minutes. At this time, individuals can relax, meditate, sleep, listen to music, etc. The practitioner may monitor if and how the pulse has changed and add or remove needles. After the needles are removed, the practitioner will determine the course of treatment. Depending on how chronic or severe the condition is, they may recommend several acupuncture pain management treatments over the course of several weeks.
Chiropractic Care For Healing After Trauma
References
World Health Organization. (2021). WHO benchmarks for the practice of acupuncture.
Hao, J. J., & Mittelman, M. (2014). Acupuncture: past, present, and future. Global advances in health and medicine, 3(4), 6–8. doi.org/10.7453/gahmj.2014.042
Johns Hopkins Medicine. (2024). Acupuncture.
Lu, L., Zhang, Y., Tang, X., Ge, S., Wen, H., Zeng, J., Wang, L., Zeng, Z., Rada, G., Ávila, C., Vergara, C., Tang, Y., Zhang, P., Chen, R., Dong, Y., Wei, X., Luo, W., Wang, L., Guyatt, G., Tang, C., … Xu, N. (2022). Evidence on acupuncture therapies is underused in clinical practice and health policy. BMJ (Clinical research ed.), 376, e067475. doi.org/10.1136/bmj-2021-067475
Liu, S., Wang, Z. F., Su, Y. S., Ray, R. S., Jing, X. H., Wang, Y. Q., & Ma, Q. (2020). Somatotopic Organization and Intensity Dependence in Driving Distinct NPY-Expressing Sympathetic Pathways by Electroacupuncture. Neuron, 108(3), 436–450.e7. doi.org/10.1016/j.neuron.2020.07.015
National Center for Complementary and Integrative Health. (2022). Acupuncture: what you need to know.
Bäumler, P., Zhang, W., Stübinger, T., & Irnich, D. (2021). Acupuncture-related adverse events: systematic review and meta-analyses of prospective clinical studies. BMJ open, 11(9), e045961. doi.org/10.1136/bmjopen-2020-045961
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine