Back Clinic Sciatica Nerve Pain Chiropractic, Physical Therapy Treatment Team. The common cause is a bulging or ruptured disc (herniated disc) in the spine pressing against the nerve roots that lead to the sciatic nerve. Sciatica nerve pain can also be a symptom of other conditions affecting the spine, such as narrowing of the spinal canal (spinal stenosis), bone spurs (small, bony growths that form along joints) caused by arthritis, or nerve root compression (pinched nerve) caused by injury. In rare cases, sciatica can also be caused by conditions that do not involve the spine, i.e. tumors or pregnancy.
What are the symptoms?
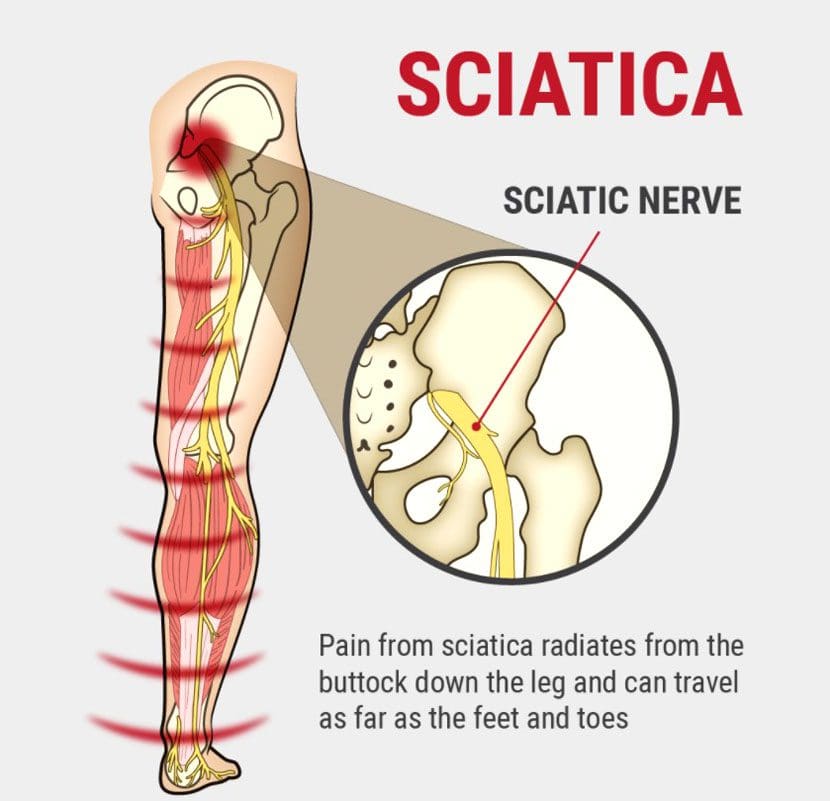
Pain that begins in your back or buttock and moves down your leg and may move into the foot. Weakness, tingling, or numbness in the leg may also occur.
Sitting, standing for a long time, and movements that cause the spine to flex (such as knee-to-chest exercises) may make symptoms worse.
Walking, lying down, and movements that extend the spine (such as press-ups) may relieve symptoms.For answers to any questions you may have please call Dr. Jimenez at 915-850-0900
Disc bulge and disc herniation are some of the most common conditions affecting the spine of both young and middle-aged patients. It is estimated that approximately 2.6% of the US population annually visits a clinician to treat spinal disorders. Roughly $ 7.1 billion alone is lost due to the time away from work.
Disc herniation is when the whole or part of the nucleus pulposus is protruded through the torn or weakened outer annulus fibrosus of the intervertebral disc. This is also known as the slipped disc and frequently occurs in the lower back, sometimes also affecting the cervical region. Herniation of the intervertebral disc is defined as a localized displacement of disc material with 25% or less of the disc circumference on an MRI scan, according to the North American Spine Society 2014. The herniation may consist of nucleus pulposus, annulus fibrosus, apophyseal bone or osteophytes, and the vertebral endplate cartilage in contrast to disc bulge.
There are also mainly two types of disc herniation. Disc protrusion is when a focal or symmetrical extension of the disc comes out of its confines in the intervertebral space. It is situated at the intervertebral disc level, and its outer annular fibers are intact. A disc extrusion is when the intervertebral disc extends above or below the adjacent vertebrae or endplates with a complete annular tear. In this type of disc extrusion, a neck or base is narrower than the dome or the herniation.
A disc bulge is when the outer fibers of the annulus fibrosus are displaced from the margins of the adjacent vertebral bodies. Here, the displacement is more than 25% of the circumference of the intervertebral disc. It also does not extend below or above the margins of the disc because the annulus fibrosus attachment limits it. It differs from disc herniation because it involves less than 25% of the disc’s circumference. Usually, the disc bulge is a gradual process and is broad. The disc bulge can be divided into two types. In a circumferential bulge, the whole disc circumference is involved. More than 90 degrees of the rim is involved asymmetrically in asymmetrical bulging.
Normal Intervertebral Disc Anatomy
Before going into detail about the definition of disc herniation and disc bulge, we need to look at the standard intervertebral disc. According to spine guidelines in 2014, a standard disc is something that has a classic shape without any evidence of degenerative disc changes. Intervertebral discs are responsible for one-third to one-fourth of the height of the spinal column.
One intervertebral disc is about 7 -10 mm thick and measures 4 cm in anterior-posterior diameter in the lumbar region of the spine. These spinal discs are located between two adjacent vertebral bodies. However, no discs can be found between the atlas and axis and the coccyx. About 23 discs are found in the spine, with six in the cervical spine, 12 in the thoracic spine, and only five in the lumbar spine.
Intervertebral discs are made of fibro cartilages, forming a fibrocartilaginous joint. The outer ring of the intervertebral disc is known as the annulus fibrosus, while the inner gel-like structure in the center is known as the nucleus pulposus. The cartilage endplates sandwich the nucleus pulposus superiorly and inferiorly. The annulus fibrosus comprises concentric collagen fiber sheets arranged in a radial tire-like structure into lamellae. The fibers are attached to the vertebral endplates and oriented at different angles. With their cartilaginous part, the endplates anchor the discs in their proper place.
The nucleus pulposus is composed of water, collagen, and proteoglycans. Proteoglycans attract and retain moisture, giving the nucleus pulposus a hydrated gel-like consistency. Interestingly, throughout the day, the amount of water found in the nucleus pulposus varies according to the person’s level of activity. This feature in the intervertebral disc serves as a cushion or a spinal shock-absorbing system to protect the adjacent vertebra, spinal nerves, spinal cord, brain, and other structures against various forces. Although the individual movement of the intervertebral discs is limited, some form of vertebral motion like flexion and extension is still possible due to the features of the intervertebral disc.
Effect of Intervertebral Disc Morphology on Structure and Function
The type of components present in the intervertebral disc and how it is arranged determine the morphology of the intervertebral disc. This is important in how effectively the disc does its function. As the disc is the most important element which bears the load and allows movement in the otherwise rigid spine, the constituents it is made up of have a significant bearing.
The complexity of the lamellae increases with advancing age as a result of the synthetic response of the intervertebral disc cells to the variations in the mechanical load. These changes in lamellae with more bifurcations, interdigitation and irregular size and number of lamellar bands will lead to the altered bearing of weight. This in turn establishes a self-perpetuated disruption cycle leading to the destruction of the intervertebral discs. Once this process is started it is irreversible. As there is an increased number of cells, the amount of nutrition the disc requires is also increasingly changing the normal concentration gradient of both metabolites and nutrients. Due to this increased demand, the cells may also die increasingly by necrosis or apoptosis.
Human intervertebral discs are avascular and hence the nutrients are diffused from the nearby blood vessels in the margin of the disc. The main nutrients; oxygen and glucose reach the cells in the disc through diffusion according to the gradient determined by the rate of transport to the cells through the tissues and the rate of demand. Cells also increasingly produce lactic acid as a metabolic end product. This is also removed via the capillaries and venules back to the circulation.
Since diffusion depends on the distance, the cells lying far from the blood capillaries can have a reduced concentration of nutrients because of the reduced supply. With disease processes, the normally avascular intervertebral disc can become vascular and innervated in degeneration and in disease processes. Although this may increase the oxygen and nutrient supply to the cells in the disc, this can also give rise to many other types of cells that are normally not found in the disc with the introduction of cytokines and growth factors.
The morphology of the intervertebral disc in different parts of the spine also varies although many clinicians base the clinical theories based on the assumption that both cervical and lumbar intervertebral discs have the same structure. The height of the disc was the minimum in the T4-5 level of the thoracic column probably due to the fact that thoracic intervertebral discs are less wedge-shaped than those of cervical and lumbar spinal regions.
From the cranial to caudal direction, the cross-sectional area of the spine increased. Therefore, by the L5-S1 level, the nucleus pulposus was occupying a higher proportion of the intervertebral disc area. The cervical discs have an elliptical shape on cross-section while the thoracic discs had a more circular shape. The lumbar discs also have an elliptical shape though it is more flattened or re-entrant posteriorly.
What is a Disc Bulge?
The bulging disc is when the disc simply bulges outside the intervertebral disc space it normally occupies without the rupture of the outer annulus fibrosus. The bulging area is quite large when compared to a herniated disc. Moreover, in a herniated disc, the annulus fibrosus ruptures or cracks. Although disc bulging is more common than disc herniation, it causes little or no pain to the patient. In contrast, the herniated disc causes a lot of pain.
Causes for Disc Bulging
A bulging disc can be due to several causes. It can occur due to normal age-related changes such as those seen in degenerative disc disease. The aging process can lead to structural and biochemical changes in the intervertebral discs and lead to reduced water content in the nucleus pulposus. These changes can make the patient vulnerable to disc bulges with only minor trauma. Some unhealthy lifestyle habits such as a sedentary lifestyle and smoking can potentiate this process and give rise to more severe changes with the weakening of the disc.
General wear and tear due to repeated microtrauma can also weaken the disc and give rise to disc bulging. This is because when the discs are strained, the normal distribution of weight loading changes. Accumulated micro-trauma over a long period of time can occur in bad posture. Bad posture when sitting, standing, sleeping, and working can increase the pressure in the intervertebral discs.
When a person maintains a forward bending posture, it can lead to overstretching and eventually weakness of the posterior part of the annulus fibrosus. Over time, the intervertebral disc can bulge posteriorly. In occupations that require frequent and repetitive lifting, standing, driving, or bending, the bulging disc may be an occupational hazard. Improper lifting up of items, and improper carrying of heavy objects can also increase the pressure on the spine and lead to disc bulges eventually.
The bulging intervertebral discs usually occur over a long period of time. However, the discs can bulge due to acute trauma too. The unexpected sudden mechanical load can damage the disc resulting in micro-tears. After an accident, the disc can become weakened causing long-term microdamage ultimately leading to bulging of the disc. There may also be a genetic component to the disc bulging. The individual may have a reduced density of elastin in the annulus fibrosus with increased susceptibility to disc diseases. Other environmental facts may also play a part in this disease process.
Symptoms of Disc Bulging
As mentioned previously, bulging discs do not cause pain and even if they do the severity is mild. In the cervical region, the disease will cause pain running down the neck, deep pain in the shoulder region, pain radiating along the upper arm, and forearm up to the fingers.
This may give rise to a diagnostic dilemma as to whether the patient is suffering from a myocardial infarction as the site of referred pain and the radiation is similar. Tingling feeling on the neck may also occur due to the bulging disc.
In the thoracic region, there may be pain in the upper back that radiates to the chest or the upper abdominal region. This may also suggest upper gastrointestinal, lung, or cardiac pathology and hence need to be careful when analyzing these symptoms.
The bulging discs of the lumbar region may present as lower back pain and tingling feeling in the lower back region of the spine. This is the most common site for disc bulges since this area holds the weight of the upper body. The pain or the discomfort can spread through the gluteal area, thighs, and to the feet. There may also be muscle weakness, numbness or tingling sensation. When the disc presses on the spinal cord, the reflexes of both legs can increase leading to spasticity.
Some patients may even have paralysis from the waist down. When the bulging disc compresses on the cauda equine, the bladder and bowel functions can also change. The bulging disc can press on the sciatic nerve leading to sciatica where the pain radiates in one leg from the back down to the feet.
The pain from the bulging disc can get worse during some activities as the bulge can then compress on some of the nerves. Depending on what nerve is affected, the clinical features can also vary.
Diagnosis of Disc Bulging
The diagnosis may not be apparent from clinical history due to similar presentations in more serious problems. But the chronic nature of the disease may give some clues. Complete history and a physical examination need to be done to rule out myocardial infarction, gastritis, gastro-oesophageal reflux disease, and chronic lung pathology.
MRI of Disc Bulge
Investigations are necessary for the diagnosis. X-ray spine is performed to look for gross pathology although it may not show the bulging disc directly. There may be indirect findings of disk degeneration such as osteophytes in the endplates, gas in the disc due to the vacuum phenomenon, and the loss of height of the intervertebral disc. In the case of moderate bulges, it may sometimes appear as non-focal intervertebral disc material that is protruded beyond the borders of the vertebra which is broad-based, circumferential, and symmetrical.
Magnetic resonance imaging or MRI can exquisitely define the anatomy of the intervertebral discs especially the nucleus pulposus and its relationships. The early findings seen on MRI in disc bulging include the loss of normal concavity of the posterior disc. The bulges can be seen as broad-based, circumferential, and symmetrical areas. In moderate bulging, the disc material will protrude beyond the borders of the vertebrae in a non-focal manner. Ct myelogram may also give detailed disc anatomy and may be useful in the diagnosis.
Treatment of Disc Bulging
The treatment for the bulging disc can be conservative, but sometimes surgery is required.
Conservative Treatment
When the disc bulging is asymptomatic, the patient does not need any treatment since it does not pose an increased risk. However, if the patient is symptomatic, the management can be directed at relieving the symptoms. The pain is usually resolved with time. Till then, potent pain killers such as non-steroidal anti-inflammatory drugs like ibuprofen should be prescribed. In unresolved pain, steroid injections can also be given to the affected area and if it still does not work, the lumbar sympathetic block can be tried in most severe cases.
The patient can also be given the option of choosing alternative therapies such as professional massage, physical therapy, ice packs, and heating pads which may alleviate symptoms. Maintaining correct posture, tapes, or braces to support the spine are used with the aid of a physiotherapist. This may fasten the recovery process by avoiding further damage and keeping the damaged or torn fibers in the intervertebral disc without leakage of the fluid portion of the disc. This helps maintain the normal structure of the annulus and may increase the recovery rate. Usually, the painful symptoms which present initially get resolved over time and lead to no pain. However, if the symptoms get worse steadily, the patient may need surgery
If the symptoms are resolved, physiotherapy can be used to strengthen the muscles of the back with the use of exercises. Gradual exercises can be used for the return of function and for preventing recurrences.
Surgical Treatment
When conservative therapy does not work with a few months of treatment, surgical treatment can be considered. Most would prefer minimally invasive surgery which uses advanced technology to correct the intervertebral disc without having to grossly dissect the back. These procedures such as microdiscectomy have a lower recovery period and reduced risk of scar formation, major blood loss, and trauma to adjacent structures when compared to open surgery.
Previously, laminectomy and discectomy have been a mainstay of treatment. However, due to the invasiveness of the procedure and due to increased damage to the nerves these procedures are currently abandoned by many clinicians for disc bulging.
Disc bulging in the thoracic spine is being treated surgically with costotransversectomy where a section of the transverse process is resected to allow access to the intervertebral disc. The spinal cord and spinal nerves are decompressed by using thoracic decompression by removing a part of the vertebral body and making a small opening. The patient may also need a spinal fusion later on if the removed spinal body was significant.
Video-assisted thoracoscopic surgery can also be used where only a small incision is made and the surgeon can perform the surgery with the assistance of the camera. If the surgical procedure involved removing a large portion of the spinal bone and disc material, it may lead to spinal instability. This may need bone grafting to replace the lost portion with plates and screws to hold them in place.
What is a Disc Herniation?
As mentioned in the first section of this article, disc herniation occurs when there is disc material displaces beyond the limits of the intervertebral disc focally. The disc space consists of endplates of the vertebral bodies superiorly and inferiorly while the outer edges of the vertebral apophyses consist of the peripheral margin. The osteophytes are not considered a disc margin. There may be irritation or compression of the nerve roots and dural sac due to the volume of the herniated material leading to pain. When this occurs in the lumbar region, this is classically known as sciatica. This condition has been mentioned since ancient times although a connection between disc herniation and sciatica was made only in the 20th century. Disc herniation is one of the commonest diagnoses seen in the spine due to degenerative changes and is the commonest cause of spinal surgery.
Classifications of Disc Herniation
There are many classifications regarding intervertebral disc herniation. In focal disc herniation, there is a localized displacement of the disc material in the horizontal or axial plane. In this type, only less than 25% of the circumference of the disc is involved. In broad-based disc herniation, about 25 – 50 % of the disc circumference is herniated. The disc bulge is when 50 – 100 % of the disc material is extended beyond the normal confines of the intervertebral space. This is not considered a form of disc herniation. Furthermore, the intervertebral disc deformities associated with severe cases of scoliosis and spondylolisthesis are not classified as a herniation but rather adaptive changes of the contour of the disc due to the adjacent deformity.
Depending on the contour of the displaced material, the herniated discs can be further classified as protrusions and extrusions. In disc protrusion, the distance measured in any plane involving the edges of the disc material beyond intervertebral disc space (the highest measure is taken) is lower than the distance measured in the same plane between the edges of the base.
Imaging can show the disc displacement as a protrusion on the horizontal section and as an extrusion on the sagittal section due to the fact that the posterior longitudinal ligament contains the disc material that is displaced posteriorly. Then the herniation should be considered an extrusion. Sometimes the intervertebral disc herniation can occur in the craniocaudal or vertical direction through a defect in the vertebral body endplates. This type of herniation is known as intravertebral herniation.
The disc protrusion can also be divided into two focal protrusion and broad-based protrusion. In focal protrusion, the herniation is less than 25% of the circumference of the disc whereas, in broad-based protrusion, the herniated disc consists of 25 – 50 % of the circumference of the disc.
In disc extrusion, it is diagnosed if any of the two following criteria are satisfied. The first one is; that the distance measured between the edges of the disc material that is beyond the intervertebral disc space is greater than the distance measured in the same plane between the edges of the base. The second one is; that the material in the intervertebral disc space and material beyond the intervertebral disc space is having a lack continuity.
This can be further characterized as sequestrated which is a subtype of the extruded disc. It is called disc migration when disk material is pushed away from the site of extrusion without considering whether there is continuity of disc or not. This term is useful in interpreting imaging modalities as it is often difficult to show continuity in imaging.
The intervertebral disc herniation can be further classified as contained discs and discs that are unconfined. The term contained disc is used to refer to the integrity of the peripheral annulus fibrosus which is covering the intervertebral disc herniation. When fluid is injected into the intervertebral disc, the fluid does not leak into the vertebral canal in herniations that are contained.
Sometimes there are displaced disc fragments that are characterized as free. However, there should be no continuity between disc material and the fragment and the original intervertebral disc for it to be called a free fragment or a sequestered one. In a migrated disc and in a migrated fragment, there is an extrusion of disc material through the opening in the annulus fibrosus with a displacement of the disc material away from the annulus.
Even though some fragments that are migrated can be sequestered the term migrated means just to the position and it is not referred to the continuity of the disc. The displaced intervertebral disc material can be further described with regard to the posterior longitudinal ligament as submembranous, subcapsular, subligamentous, extra ligamentous, transligamentous, subcapsular, and perforated.
The spinal canal can also get affected by an intervertebral disc herniation. This compromise of the canal can also be classified as mild, moderate, and severe depending on the area that is compromised. If the canal at that section is compromised only less than one third, it is called mild whereas if it is only compromised less than two-thirds and more than one third it is considered moderate. In a severe compromise, more than two-thirds of the spinal canal is affected. For the foraminal involvement, this same grading system can be applied.
The displaced material can be named according to the position that they are in the axial plane from the center to the right lateral region. They are termed as central, right central, right subarticular, right foraminal, and right extraforaminal. The displaced intervertebral disc material’s composition can be further classified as gaseous, liquefied, desiccated, scarred, calcified, ossified, bony, nuclear, and cartilaginous.
Before going into detail on how to diagnose and treat intervertebral disc herniation, let us differentiate how cervical disc herniation differs from lumbar herniation since they are the most common regions to undergo herniation.
Cervical Disc Herniation vs. Thoracic Disc Herniation vs Lumbar Disc Herniation
Lumbar disc herniation is the most commonest type of herniation found in the spine which is approximately 90% of the total. However, cervical disc herniation can also occur in about one-tenth of patients. This difference is mainly due to the fact that the lumbar spine has more pressure due to the increased load. Moreover, it has comparatively large intervertebral disc material. The most common sites of intervertebral disc herniation in the lumbar region are L 5 – 6, in the Cervical region between C7, and in the thoracic region T12.
Cervical disc herniation can occur relatively commonly because the cervical spine acts as a pivoting point for the head and it is a vulnerable area for trauma and therefore prone to damage in the disc. Thoracic disc herniation occurs more infrequently than any of the two. This is due to the fact that thoracic vertebrae are attached to the ribs and the thoracic cage which limits the range of movement in the thoracic spine when compared to the cervical and lumbar spinal discs. However, thoracic intervertebral disc herniation can still occur.
Cervical disc herniation gives rise to neck pain, shoulder pain, pain radiating from the neck to the arm, tingling, etc. Lumbar disc herniation can similarly cause lower back pain as well as pain, tingling, numbness, and muscle weakness seen in the lower limbs. Thoracic disc herniation can give rise to pain in the upper back radiating to the torso.
Epidemiology
Although disc herniation can occur in all age groups, it predominantly occurs between the fourth and fifth decade of life with the mean age of 37 years. There have been reports that estimate the prevalence of intervertebral disc herniation to be 2 – 3 % of the general population. It is more commonly seen in men over 35 years with a prevalence of 4.8% and while in women this figure is around 2.5%. Due to its high prevalence, it is considered a worldwide problem as it is also associated with significant disability.
Risk Factors
In most instances, a herniated disc occurs due to the natural aging process in the intervertebral disc. Due to the disc degeneration, the amount of water that was previously seen in the intervertebral disc gets dried out leading to the shrinking of the disc with the narrowing of the intervertebral space. These changes are markedly seen in degenerative disc disease. In addition to these gradual changes due to normal wear and tear, other factors may also contribute to increasing the risk of intervertebral disc herniation.
Being overweight can increase the load on the spine and increase the risk of herniation. A sedentary life can also increase the risk and therefore an active lifestyle is recommended in preventing this condition. Improper posture with prolonged standing, sitting, and especially driving can put a strain on the intervertebral discs due to the additional vibration from the vehicle engine leading to microtrauma and cracks in the disc. The occupations which require constant bending, twisting, pulling and lifting can put a strain on the back. Improper weight lifting techniques are one of the major reasons.
When back muscles are used in lifting heavy objects instead of lifting with the legs and twisting while lifting can make the lumbar discs more vulnerable to herniation. Therefore patients should always be advised to lift weights with their legs and not the back. Smoking has been thought to increase disc herniation by reducing the blood supply to the intervertebral disc leading to degenerative changes of the disc.
Although the above factors are frequently assumed to be the causes for disc herniation, some studies have shown that the difference in risk is very small when this particular population was compared with the control groups of the normal population.
There have been several types of research done on genetic predisposition and intervertebral disc herniation. Some of the genes that are implicated in this disease include vitamin D receptor (VDR) which is a gene that codes for the polypeptides of important collagen called collagen IX (COL9A2).
Another gene called the human aggrecan gene (AGC) is also implicated as it codes for proteoglycans which is the most important structural protein found in the cartilage. It supports the biochemical and mechanical function of the cartilage tissue and hence when this gene is defective, it can predispose an individual to intervertebral disc herniation.
Apart from these, there are many other genes that are being researched due to the association between disc herniation such as matrix metalloproteinase (MMP) cartilage intermediate layer protein, thrombospondin (THBS2), collagen 11A1, carbohydrate sulfotransferase, and asporin (ASPN). They may also be regarded as potential gene markers for lumbar disc disease.
Pathogenesis of Sciatica and Disc Herniation
The sciatic pain originated from the extruded nucleus pulposus inducing various phenomena. It can directly compress the nerve roots leading to ischemia or without it, mechanically stimulate the nerve endings of the outer portion of the fibrous ring and release inflammatory substances suggesting its multifactorial origin. When the disc herniation causes mechanical compression of the nerve roots, the nerve membrane is sensitized to pain and other stimuli due to ischemia. It has been shown that in sensitized and compromised nerve roots, the threshold for neuronal sensitization is around half of that of a normal and non-compromised nerve root.
The inflammatory cell infiltration is different in extruded discs and non-extruded discs. Usually, in non-extruded discs, the inflammation is less. The extruded disc herniation causes the posterior longitudinal ligament to rupture which exposes the herniated part to the vascular bed of the epidural space. It is believed that inflammatory cells are originating from these blood vessels situated in the outermost part of the intervertebral disc.
These cells may help secrete substances that cause inflammation and irritation of the nerve roots causing sciatic pain. Therefore, extruded herniations are more likely to cause pain and clinical impairment than those that are contained. In contained herniations, the mechanical effect is predominant while in the unconfined or the extruded discs the inflammatory effect is predominant.
Clinical Disc Herniation and What to Look for in the History
The symptoms of the disc herniation can vary a great deal depending on the location of the pain, the type of herniation, and the individual. Therefore, history should focus on the analysis of the main complaint among the many other symptoms.
The chief complaint can be neck pain in cervical disc herniation and there can be referred pain in the arms, shoulders, neck, head, face, and even the lower back region. However, it is most commonly referred to as the interscapular region. The radiation of pain can occur according to the level at the herniation is taking place. When the nerve roots of the cervical region are affected and compressed, there can be sensory, and motor changes with changes in the reflexes.
The pain that occurs due to nerve root compression is called radicular pain and it can be described as deep, aching, burning, dull, achy, and electric depending on whether there is mainly motor dysfunction or sensory dysfunction. In the upper limb, the radicular pain can follow a dermatomal or myotomal pattern. Radiculopathy usually does not accompany neck pain. There can be unilateral as well as bilateral symptoms. These symptoms can be aggravated by activities that increase the pressure inside the intervertebral discs such as the Valsalva maneuver and lifting.
Driving can also exacerbate pain due to disc herniation due to stress because of vibration. Some studies have shown that shock loading and stress from vibration can cause a mechanical force to exacerbate small herniations but flexed posture had no influence. Similarly, activities that decrease intradiscal pressure can reduce the symptoms such as lying down.
The main complaint in lumbar disc herniation is lower back pain. Other associated symptoms can be a pain in the thigh, buttocks, and anogenital region which can radiate to the foot and toe. The main nerve affected in this region is the sciatic nerve causing sciatica and its associated symptoms such as intense pain in the buttocks, leg pain, muscle weakness, numbness, impairment of sensation, hot and burning or tingling sensation in the legs, dysfunction of gait, impairment of reflexes, edema, dysesthesia or paresthesia in the lower limbs. However, sciatica can be caused by causes other than herniation such as tumors, infection, or instability which need to be ruled out before arriving at a diagnosis.
The herniated disc can also compress on the femoral nerve and can give rise to symptoms such as numbness, tingling sensation in one or both legs, and a burning sensation in the legs and hips. Usually, the nerve roots that are affected in herniation in the lumbar region are the ones exiting below the intervertebral disc. It is thought that the level of the nerve root irritation determines the distribution of leg pain. In herniations at the third and fourth lumbar vertebral levels, the pain may radiate to the anterior thigh or the groin. In radiculopathy at the level of the fifth lumbar vertebra, the pain may occur in the lateral and anterior thigh region. In herniations at the level of the first sacrum, the pain may occur in the bottom of the foot and the calf. There can also be numbness and tingling sensation occurring in the same area of distribution. The weakness in the muscles may not be able to be recognized if the pain is very severe.
When changing positions the patient is often relieved from pain. Maintaining a supine position with the legs raised can improve the pain. Short pain relief can be brought by having short walks while long walks, standing for prolonged periods, and sitting for extended periods of time such as in driving can worsen the pain.
The lateral disc herniation is seen in foraminal and extraforaminal herniations and they have different clinical features to that of medial disc herniation seen in subarticular and central herniations. The lateral intervertebral disc herniations can when compared to medial herniations more directly irritate and mechanically compress the nerve roots that are exiting and the dorsal root ganglions situated inside the narrowed spinal canal.
Therefore, lateral herniation is seen more frequently in older age with more radicular pain and neurological deficits. There is also more radiating leg pain and intervertebral disc herniations in multiple levels in the lateral groups when compared to medial disc herniations.
The herniated disc in the thoracic region may not present with back pain at all. Instead, there are predominant symptoms due to referred pain in the thorax due to irritation of nerves. There can also be predominant pain in the body that travels to the legs, tingling sensation and numbness in one or both legs, muscle weakness, and spasticity of one or both legs due to exaggerated reflexes.
The clinician should look out for atypical presentations as there could be other differential diagnoses. The onset of symptoms should be inquired about to determine whether the disease is acute, sub-acute, or chronic in onset. Past medical history has to be inquired about in detail to exclude red flag symptoms such as pain that occurs at night without activity which can be seen in pelvic vein compression, and non-mechanical pain which may be seen in tumors or infections.
If there is a progressive neurological deficit, with bowel and bladder involvement is there, it is considered a neurological emergency and urgently investigated because cauda equine syndrome may occur which if untreated, can lead to permanent neurological deficit.
Getting a detailed history is important including the occupation of the patient as some activities in the job may be exacerbating the patient’s symptoms. The patient should be assessed regarding which activities he can and cannot do.
Differential Diagnosis
Degenerative disc disease
Mechanical pain
Myofascial pain leading to sensory disturbances and local or referred pain
Hematoma
Cyst leading to occasional motor deficits and sensory disturbances
Spondylosis or spondylolisthesis
Discitis or osteomyelitis
Malignancy, neurinoma or mass lesion causing atrophy of thigh muscles, glutei
Spinal stenosis is seen mainly in the lumbar region with mild low back pain, motor deficits, and pain in one or both legs.
An epidural abscess can cause symptoms similar to radicular pain involving spinal disc herniation
Aortic aneurysm which can cause low back pain and leg pain due to compression can also rupture and lead to hemorrhagic shock.
Hodgkin’s lymphoma in advanced stages can lead to space-occupying lesions in the spinal column leading to symptoms like that of intervertebral disc herniation
Tumors
Pelvic endometriosis
Facet hypertrophy
Lumbar nerve root schwannoma
Herpes zoster infection results in inflammation along with the sciatic or lumbosacral nerve roots
Examination in Disc Herniation
Complete physical examination is necessary to diagnose intervertebral disc herniation and exclude other important differential diagnoses. The range of motion has to be tested but may have a poor correlation with disc herniation as it is mainly reduced in elderly patients with a degenerative disease and due to disease of the joints.
A complete neurological examination is often necessary. This should test muscle weakness and sensory weakness. In order to detect muscle weakness in small toe muscles, the patient can be asked to walk on tiptoe. The strength of muscle can also be tested by comparing the strength to that of the clinician. There may be dermatomal sensory loss suggesting the respective nerve root involvement. The reflexes may be exaggerated or sometimes maybe even absent.
There are many neurologic examination maneuvers described in relation to intervertebral disc herniation such as the Braggart sign, flip the sign, Lasegue rebound sign, Lasegue differential sign, Mendel Bechterew sign, Deyerle sign both legs or Milgram test, and well leg or Fajersztajin test. However, all these are based on testing the sciatic nerve root tension by using the same principles in the straight leg raising test. These tests are used for specific situations to detect subtle differences.
Nearly almost all of them depend on the pain radiating down the leg and if it occurs above the knee it is assumed to be due to a neuronal compressive lesion and if the pain goes below the knee, it is considered to be due to the compression of the sciatic nerve root. For lumbar disc herniation detection, the most sensitive test is considered to be radiating pain occurring down the leg due to provocation.
In the straight leg raising test also called the Lasegue’s sign, the patient stays on his or her back and keeps the legs straight. The clinician then lifts the legs by flexing the hip while keeping the knee straight. The angle at which the patient feels pain going down the leg below the knee is noted. In a normal healthy individual, the patient can flex the hip to 80- 90? without having any pain or difficulty.
However, if the angle is just 30 -70? degrees, it is suggestive of lumbar intervertebral disc herniation at the L4 to S1 nerve root levels. If the angle of hip flexion without pain is less than 30 degrees, it usually indicates some other causes such as tumor of the gluteal region, gluteal abscess, spondylolisthesis, disc extrusion, and protrusion, malingering patient, and acute inflammation of the dura mater. If pain with hip flexion occurs at more than 70 degrees, it may be due to tightness of the muscles such as gluteus maximus and hamstrings, tightness of the capsule of the hip joint, or pathology of sacroiliac or hip joints.
The reverse straight leg raising test or hip extension test can be used to test higher lumbar lesions by stretching the nerve roots of the femoral nerve which is similar to the straight leg raising test. In the cervical spine, in order to detect stenosis of the foramina, the Spurling test is done and is not specific to cervical intervertebral disc herniation or tension of the nerve roots. The Kemp test is the analogous test in the lumbar region to detect foraminal stenosis. Complications due to the disc herniation include careful examination of the hip region, digital rectal examination, and urogenital examination is needed.
Investigation of Disc Herniation
For the diagnosis of intervertebral disc herniation, diagnostic tests such as Magnetic resonance imaging (MRI), Computed tomography (CT), myelography, and plain radiography can be used either alone or in combination with other imaging modalities. Objective detection of disc herniation is important because only after such a finding the surgical intervention is even considered. Serum biochemical tests such as prostate-specific antigen (PSA) level, Alkaline phosphatize value, erythrocyte sedimentation rate (ESR), urine analysis for Bence Jones protein, serum glucose level, and serum protein electrophoresis may also be needed in specific circumstances guided by history.
Magnetic Resonance Imaging (MRI)
MRI is considered the best imaging modality in patients with history and physical examination findings suggestive of lumbar disc herniation associated with radiculopathy according to North American Spinal Society guidelines in 2014. The anatomy of the herniated nucleus pulposus and its associated relationships with soft tissue in the adjacent areas can be delineated exquisitely by MRI in cervical, thoracic, and lumbosacral areas. Beyond the confines of the annulus, the herniated nucleus can be seen as a focal, asymmetric disc material protrusion on MRI.
On sagittal T2 weighted images, the posterior annulus is usually seen as a high signal intensity area due to radial annular tear associated with the herniation of the disc although the herniated nucleus is itself hypointense. The relationship between the herniated nucleus and degenerated facets with the nerve roots which are exiting through the neural foramina are well-demarcated on sagittal images of MRI. Free fragments of the intervertebral disc can also be distinguished from MRI images.
There may be associated signs of intervertebral disc herniation on MRI such as radial tears on the annulus fibrosus which is also a sign of degenerative disc disease. There may be other telling signs such as loss of disc height, bulging annulus, and changes in the endplates. Atypical signs may also be seen with MRI such as abnormal disc locations, and lesions located completely outside the intervertebral disc space.
MRI can detect abnormalities in the intervertebral discs superiorly to other modalities although its bone imaging is a little less inferior. However, there are limitations with MRI in patients with metal implant devices such as pacemakers because the electromagnetic field can lead to abnormal functioning of the pacemakers. In patients with claustrophobia, it may become a problem to go to the narrow canal to be scanned by the MRI machine. Although some units contain open MRI, it has less magnetic power and hence delineates less superior quality imaging.
This is also a problem in children and anxious patients undergoing MRI because good image quality depends on the patient staying still. They may require sedation. The contrast used in MRI which is gadolinium can induce nephrogenic systemic fibrosis in patients who had pre-existing renal disease. MRI is also generally avoided in pregnancy especially during the first 12 weeks although it has not been clinically proven to be hazardous to the fetus. MRI is not very useful when a tumor contains calcium and in distinguishing edema fluid from tumor tissue.
Computed Tomography (CT)
CT scanning is also considered another good method to assess spinal disc herniation when MRI is not available. It is also recommended as a first-line investigation in unstable patients with severe bleeding. CT scanning is superior to myelography although when the two are combined, it is superior both of them. CT scans can show calcification more clearly and sometimes even gas in images. In order to achieve a superior imaging quality, the imaging should be focused on the site of pathology and thin sections taken to better determine the extent of the herniation.
However, a CT scan is difficult to be used in patients who have already undergone laminectomy surgical procedures because the presence of scar tissue and fibrosis causes the identification of the structures difficult although bony changes and deformity in nerve sheath are helpful in making a diagnosis.
The herniated intervertebral discs in the cervical disc can be identified by studying the uncinate process. It is usually projected posteriorly and laterally to the intervertebral discs and superiorly to the vertebral bodies. The uncinate process undergoes sclerosis, and hypertrophy when there is an abnormal relationship between the uncinate process and adjacent structures as seen in degenerative disc disease, intervertebral disc space narrowing, and general wear and tear.
Myelopathy can occur when the spinal canal is affected due to disc disease. Similarly, when neural foramina are involved, radiculopathy occurs. Even small herniated discs and protrusions can cause impingement of the dural sac because the cervical epidural space is narrowed naturally. The intervertebral discs have attenuation a little bit greater than the sac characterized in the CT scan.
In the thoracic region, a CT scan can diagnose an intervertebral disc herniation with ease due to the fact that there is an increased amount of calcium found in the thoracic discs. Lateral to the dural sac, the herniated disc material can be seen on CT as a clearly defined mass that is surrounded by epidural fat. When there is a lack of epidural fat, the disc appears as a higher attenuated mass compared to the surrounding.
Radiography
Plain radiography is not needed in diagnosing herniation of the intervertebral discs, because plain radiographs cannot detect the disc and therefore are used to exclude other conditions such as tumors, infections, and fractures.
In myelography, there may be deformity or displacement of the extradural contrast-filled thecal sac seen in herniation of the disc. There may also be features in the affected nerve such as edema, elevation, deviation, and amputation of the nerve root seen in the myelography image.
Diskography
In this imaging modality, the contrast medium is injected into the disc in order to assess the disc morphology. If pain occurs following injection that is similar to the discogenic pain, it suggests that that disc is the source of the pain. When a CT scan is also performed immediately after discography, it is helpful to differentiate the anatomy and pathological changes. However, since it is an invasive procedure, it is indicated only in special circumstances when MRI and CT have failed to reveal the etiology of back pain. It has several side effects such as headache, meningitis, damage to the disc, discitis, intrathecal hemorrhage, and increased pain.
Treatment of Herniated Disc
The treatment should be individualized according to the patient-guided through history, physical examination, and diagnostic investigation findings. In most cases, the patient gradually improves without needing further intervention in about 3 – 4 months. Therefore, the patient only needs conservative therapy during this time period. Because of this reason, there are many ineffective therapies that have emerged by attributing the natural resolution of symptoms to that therapy. Therefore, conservative therapy needs to be evidence-based.
Conservative Therapy
Since the herniation of the disc has a benign course, the aim of treatment is to stimulate the recovery of neurological function, reduce pain, and facilitate early return to work and activities of daily living. The most benefits of the conservative treatment are for younger patients with hernias that are sequestered and in patients with mild neurological deficits due to small disc hernias.
Bed rest has long been considered a treatment option in herniation of the disc. However, it has been shown that bed rest has no effect beyond the first 1 or 2 days. The bed rest is regarded as counterproductive after this period of time.
In order to reduce the pain, oral non-steroidal anti-inflammatory drugs such as ibuprofen and naproxen can be used. This can relieve the pain by reducing inflammation associated with the inflamed nerve. Analgesics such as acetaminophen can also be used although they lack the anti-inflammatory effect seen in NSAIDs. The doses and the drugs should be appropriate for the age and severity of the pain in the patient. If pain is not controlled by the current medication, the clinician has to go one step up on the WHO analgesics ladder. However, the long-term use of NSAIDs and analgesics can lead to gastric ulcers, liver, and kidney problems.
In order to reduce the inflammation, other alternative methods such as applying ice in the initial period and then switching to using heat, gels, and rubs may help with the pain as well as muscle spasms. Oral muscle relaxants can also be used in relieving muscle spasms. Some of the drugs include methocarbamol, carisoprodol, and cyclobenzaprine.
However, they act centrally and cause drowsiness and sedation in patients and it does not act directly to reduce muscle spasm. A short course of oral steroids such as prednisolone for a period of 5 days in a tapering regime can be given to reduce the swelling and inflammation in the nerves. It can provide immediate pain relief within a period of 24 hours.
When the pain is not resolved adequately with maximum effective doses, the patient can be considered for giving steroid injections into the epidural space. The major indication for the steroid injection into periradicular space is discal compression causing radicular pain that is resistant to conventional medical treatment. A careful evaluation with CT or MRI scanning is required to carefully exclude extra discal causes for pain. The contraindications for this therapy include patients with diabetes, pregnancy, and gastric ulcers. Epidural puncture is contraindicated in patients with coagulation disorders and therefore the foraminal approach is used carefully if needed.
This procedure is performed under the guidance of fluoroscopy and involves injecting steroids and an analgesic into the epidural space adjacent to the affected intervertebral disc to reduce the swelling and inflammation of the nerves directly in an outpatient setting. As much as 50% of the patients experience relief after the injection although it is temporary and they might need repeat injections at 2 weekly intervals to achieve the best results. If this treatment modality becomes successful, up to 3 epidural steroidal injections can be given per year.
Physical therapy can help the patient return to his previous life easily although it does not improve the herniated disc. The physical therapist can instruct the patient on how to maintain the correct posture, walking, and lifting techniques depending on the patient’s ability to work, mobility, and flexibility.
Stretching exercises can improve the flexibility of the spine while strengthening exercises can increase the strength of the back muscles. The activities which can aggravate the condition of the herniated disc are instructed to be avoided. Physical therapy makes the transition from intervertebral disc herniation to an active lifestyle smooth. The exercise regimes can be maintained for life to improve general well-being.
The most effective conservative treatment option that is evidence-based is observation and epidural steroid injection for the relief of pain in the short-term duration. However, if the patients so desire they can use holistic therapies of their choice with acupuncture, acupressure, nutritional supplements, and biofeedback although they are not evidence-based. There is also no evidence to justify the use of trans electrical nerve stimulation (TENS) as a pain relief method.
If there is no improvement in the pain after a few months, surgery can be contemplated and the patient must be selected carefully for the best possible outcome.
Surgical Therapy
The aim of surgical therapy is to decompress the nerve roots and relieve the tension. There are several indications for surgical treatment which are as follows.
Absolute indications include cauda equina syndrome or significant paresis. Other relative indications include motor deficits that are greater than grade 3, sciatica that is not responding to at least six months of conservative treatment, sciatica for more than six weeks, or nerve root pain due to foraminal bone stenosis.
There have been many discussions over the past few years regarding whether to treat herniation of intervertebral disc disease with prolonged conservative treatment or early surgical treatment. Much research has been conducted in this regard and most of them show that the final clinical outcome after 2 years is the same although the recovery is faster with early surgery. Therefore, it is suggested that early surgery may be appropriate as it enables the patient to return to work early and thereby is economically feasible.
Some surgeons may still use traditional discectomy although many are using minimally invasive surgical techniques over recent years. Microdiscectomy is considered to be the halfway between the two ends. There are two surgical approaches that are being used. Minimally invasive surgery and percutaneous procedures are the ones that are being used due to their relative advantage. There is no place for the traditional surgical procedure known as a laminectomy.
However, there are some studies suggesting microdiscectomy is more favorable because of its both short-term and long-term advantages. In the short term, there is a reduced length of operation, reduced bleeding, relief of symptoms, and reduced complication rate. This technique has been effective even after 10 years of follow-up and therefore is the most preferred technique even now. The studies that have been performed to compare the minimally invasive technique and microdiscectomy have resulted in different results. Some have failed to establish a significant difference while one randomized control study was able to determine that microdiscectomy was more favorable.
In microdiscectomy, only a small incision is made aided by an operating microscope and the part of the herniated intervertebral disc fragment which is impinging on the nerve is removed by hemilaminectomy. Some part of the bone is also removed to facilitate access to the nerve root and the intervertebral disc. The duration of the hospital stay is minimal with only an overnight stay and observation because the patient can be discharged with minimal soreness and complete relief of the symptoms.
However, some unstable patients may need more prolonged admission and sometimes they may need fusion and arthroplasty. It is estimated that about 80 – 85 % of the patients who undergo microdiscectomy recover successfully and many of them are able to return to their normal occupation in about 6 weeks.
There is a discussion on whether to remove a large portion of the disc fragment and curetting the disc space or to remove only the herniated fragment with minimal invasion of the intervertebral disc space. Many studies have suggested that the aggressive removal of large chunks of the disc could lead to more pain than when conservative therapy is used with 28% versus 11.5 %. It may lead to degenerative disc disease in the long term. However, with conservative therapy, there is a greater risk of recurrence of around 7 % in herniation of the disc. This may require additional surgery such as arthrodesis and arthroplasty to be performed in the future leading to significant distress and economic burden.
In the minimally invasive surgery, the surgeon usually makes a tiny incision in the back to put the dilators with increasing diameter to enlarge the tunnel until it reaches the vertebra. This technique causes lesser trauma to the muscles than when seen in traditional microdiscectomy. Only a small portion of the disc is removed in order to expose the nerve root and the intervertebral disc. Then the surgeon can remove the herniated disc by the use of an endoscope or a microscope.
These minimally invasive surgical techniques have a higher advantage of lower surgical site infections and shorter hospital stays. The disc is centrally decompressed either chemically or enzymatically with the use of chymopapain, laser, or plasma (ionized gas) ablation and vaporization. It can also be decompressed mechanically by using percutaneous lateral decompression or by aspirating and sucking with a shaver such as a nucleosome. Chemopapin was shown to have adverse effects and was eventually withdrawn. Most of the above techniques have shown to be less effective than a placebo. Directed segmentectomy is the one that has shown some promise in being effective similar to microdiscectomy.
In the cervical spine, the herniated intervertebral discs are treated anteriorly. This is because the herniation occurs anteriorly and the manipulation of the cervical cord is not tolerated by the patient. The disc herniation that is due to foraminal stenosis and that is confined to the foramen are the only instances where a posterior approach is contemplated.
The minimal disc excision is an alternative to the anterior cervical spine approach. However, the intervertebral disc stability after the procedure is dependent on the residual disc. The neck pain can be significantly reduced following the procedure due to the removal of neuronal compression although significant impairment can occur with residual axial neck pain. Another intervention for cervical disc herniation includes anterior cervical interbody fusion. It is more suitable for patients with severe myelopathy with degenerative disc disease.
Complications of the Surgery
Although the risk of surgery is very low, complications can still occur. Post-operative infection is one of the commonest complications and therefore needs more vigorous infection control procedures in the theatre and in the ward. During the surgery, due to poor surgical technique, nerve damage can occur. A dural leak may occur when an opening in the lining of the nerve root causes leakage of cerebrospinal fluid which is bathing the nerve roots. The lining can be repaired during the surgery. However, headache can occur due to loss of cerebrospinal fluid but it usually improves with time without any residual damage. If blood around the nerve roots clots after the surgery, that blood clot may lead to compression of the nerve root leading to radicular pain which was experienced by the patient previously. Recurrent herniation of the intervertebral disc due to herniation of disc material at the same site is a devastating complication that can occur long term. This can be managed conservatively but surgery may be necessary ultimately.
Outcomes of the Surgery
There has been extensive research done regarding the outcome of lumbar disc herniation surgery. Generally, the results from the microdiscectomy surgery are good. There is more improvement of leg pain than back pain and therefore this surgery is not recommended for those who have only back pain. Many patients improve clinically over the first week but they may improve over the following several months. Typically, the pain disappears in the initial recovery period and it is followed by an improvement in the strength of the leg. Finally, the improvement of the sensation occurs. However, patients may complain of feeling numbness although there is no pain. The normal activities and work can be resumed over a few weeks after the surgery.
Novel Therapies
Although conservative therapy is the most appropriate therapy in treating patients, the current standard of care does not address the underlying pathology of herniation of the intervertebral discs. There are various pathways that are involved in the pathogenesis such as inflammatory, immune-mediated, and proteolytic pathways.
The role of inflammatory mediators is currently under research and it has led to the development of new therapies that are directed at these inflammatory mediators causing damage to the nerve roots. The cytokines such as TNF ? are mainly involved in regulating these processes. The pain sensitivity is mediated by serotonin receptor antagonists and ?2 adrenergic receptor antagonists.
Therefore, pharmacological therapies that target these receptors and mediators may influence the disease process and lead to a reduction in symptoms. Currently, cytokine antagonists against TNF ? and IL 1? have been tested. Neuronal receptor blockers such as sarpogrelate hydrochloride etc have been tested in both animal models and in clinical studies for the treatment of sciatica. Cell cycle modifiers that target the microglia that are thought to initiate the inflammatory cascade have been tested with the neuroprotective antibiotic minocycline.
There is also research on inhibiting the NF- kB or protein kinase pathway recently. In the future, the treatment of herniation of the intervertebral disc will be much more improved thanks to the ongoing research. (Haro, Hirotaka)
Dr. Alex Jimenez DC, MSACP, RN, CCST
A disc bulge and/or a herniated disc is a health issue that affects the intervertebral discs found in between each vertebra of the spine. Although these can occur as a natural part of degeneration with age, trauma or injury as well as repetitive overuse can also cause a disc bulge or a herniated disc. According to healthcare professionals, a disc bulge and/or a herniated disc is one of the most common health issues affecting the spine. A disc bulge is when the outer fibers of the annulus fibrosus are displaced from the margins of the adjacent vertebral bodies. A herniated disc is when a part of or the whole nucleus pulposus is protruded through the torn or weakened outer annulus fibrosus of the intervertebral disc. Treatment of these health issues focuses on reducing symptoms. Alternative treatment options, such as chiropractic care and/or physical therapy, can help relieve symptoms. Surgery may be utilized in cases of severe symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Curated by Dr. Alex Jimenez D.C., C.C.S.T.
References
Anderson, Paul A. et al. Randomized Controlled Trials Of The Treatment Of Lumbar Disk Herniation: 1983-2007. Journal Of The American Academy Of Orthopaedic Surgeons, vol 16, no. 10, 2008, pp. 566-573. American Academy Of Orthopaedic Surgeons, doi:10.5435/00124635-200810000-00002.
Fraser I (2009) Statistics on hospital-based care in the United States. Agency for Healthcare Research and Quality, Rockville
Ricci, Judith A. et al. Back Pain Exacerbations And Lost Productive Time Costs In United States Workers. Spine, vol 31, no. 26, 2006, pp. 3052-3060. Ovid Technologies (Wolters Kluwer Health), doi:10.1097/01.brs.0000249521.61813.aa.
Fardon, D.F., et al., Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology, and the American Society of Neuroradiology. Spine J, 2014. 14(11): p. 2525-45.
Costello RF, Beall DP. Nomenclature and standard reporting terminology of intervertebral disk herniation. Magn Reson Imaging Clin N Am. 2007;15 (2): 167-74, v-vi.
Roberts, S. Disc Morphology In Health And Disease. Biochemical Society Transactions, vol 30, no. 5, 2002, pp. A112.4-A112. Portland Press Ltd., doi:10.1042/bst030a112c.
Johnson, W. E. B., and S. Roberts. Human Intervertebral Disc Cell Morphology And Cytoskeletal Composition: A Preliminary Study Of Regional Variations In Health And Disease. Journal Of Anatomy, vol 203, no. 6, 2003, pp. 605-612. Wiley-Blackwell, doi:10.1046/j.1469-7580.2003.00249.x.
Gruenhagen, Thijs. Nutrient Supply And Intervertebral Disc Metabolism. The Journal Of Bone And Joint Surgery (American), vol 88, no. suppl_2, 2006, p. 30. Ovid Technologies (Wolters Kluwer Health), doi:10.2106/jbjs.e.01290.
Mercer, S.R., and G.A. Jull. Morphology Of The Cervical Intervertebral Disc: Implications For Mckenzies Model Of The Disc Derangement Syndrome. Manual Therapy, vol 1, no. 2, 1996, pp. 76-81. Elsevier BV, doi:10.1054/math.1996.0253.
KOELLER, W et al. Biomechanical Properties Of Human Intervertebral Discs Subjected To Axial Dynamic Compression. Spine, vol 9, no. 7, 1984, pp. 725-733. Ovid Technologies (Wolters Kluwer Health), doi:10.1097/00007632-198410000-00013.
Lieberman, Isador H. Disc Bulge Bubble: Spine Economics 101. The Spine Journal, vol 4, no. 6, 2004, pp. 609-613. Elsevier BV, doi:10.1016/j.spinee.2004.09.001.
Lappalainen, Anu K et al. Intervertebral Disc Disease In Dachshunds Radiographically Screened For Intervertebral Disc Calcifications. Acta Veterinaria Scandinavica, vol 56, no. 1, 2014, Springer Nature, doi:10.1186/s13028-014-0089-4.
Moazzaz, Payam et al. 80. Positional MRI: A Valuable Tool In The Assessment Of Cervical Disc Bulge. The Spine Journal, vol 7, no. 5, 2007, p. 39S. Elsevier BV, doi:10.1016/j.spinee.2007.07.097.
Vialle, Luis Roberto et al. LUMBAR DISC HERNIATION. Revista Brasileira De Ortopedia (English Edition), vol 45, no. 1, 2010, pp. 17-22. Elsevier BV, doi:10.1016/s2255-4971(15)30211-1.
Mullen, Denis et al. Pathophysiology Of Disk-Related Sciatica. I. Evidence Supporting A Chemical Component. Joint Bone Spine, vol 73, no. 2, 2006, pp. 151-158. Elsevier BV, doi:10.1016/j.jbspin.2005.03.003.
Jacobs, Wilco C. H. et al. Surgical Techniques For Sciatica Due To Herniated Disc, A Systematic Review. European Spine Journal, vol 21, no. 11, 2012, pp. 2232-2251. Springer Nature, doi:10.1007/s00586-012-2422-9.
Rutkowski, B. Combined Practice Of Electrical Stimulation For Lumbar Intervertebral Disc Herniation.Pain, vol 11, 1981, p. S226. Ovid Technologies (Wolters Kluwer Health), doi:10.1016/0304-3959(81)90487-5.
Weber, Henrik. Spine Update The Natural History Of Disc Herniation And The Influence Of Intervention.Spine, vol 19, no. 19, 1994, pp. 2234-2238. Ovid Technologies (Wolters Kluwer Health), doi:10.1097/00007632-199410000-00022.
Disk Herniation Imaging: Overview, Radiography, Computed Tomography.Emedicine.Medscape.Com, 2017,
Carvalho, Lilian Braighi et al. Hrnia De Disco Lombar: Tratamento. Acta Fisitrica, vol 20, no. 2, 2013, pp. 75-82. GN1 Genesis Network, doi:10.5935/0104-7795.20130013.
Kerr, Dana et al. What Are Long-Term Predictors Of Outcomes For Lumbar Disc Herniation? A Randomized And Observational Study. Clinical Orthopaedics And Related Research, vol 473, no. 6, 2014, pp. 1920-1930. Springer Nature, doi:10.1007/s11999-014-3803-7.
Buy, Xavier, and Afshin Gangi. Percutaneous Treatment Of Intervertebral Disc Herniation. Seminars In Interventional Radiology, vol 27, no. 02, 2010, pp. 148-159. Thieme Publishing Group, doi:10.1055/s-0030-1253513.
Haro, Hirotaka. Translational Research Of Herniated Discs: Current Status Of Diagnosis And Treatment. Journal Of Orthopaedic Science, vol 19, no. 4, 2014, pp. 515-520. Elsevier BV, doi:10.1007/s00776-014-0571-x.
As individual bodies age, the nerves and muscles begin to degenerate, especially in the lower spinal region. This can cause sciatic pain and muscle weakness. Elderly sciatica is very common as the nerves and muscles have gone through a lot. Bending, lifting, carrying, reaching, twisting, and natural wearing and tearing make the sciatic nerve and surrounding muscles prone to injury. For overweight seniors, the risk of developing sciatica is higher.
Elderly Sciatica
The main reason for elderly sciatica is that as the body ages, the discs/cartilage between the vertebrae/bones in the spine dry out, losing their cushioning ability, which can lead to the bones shifting out of place more easily, rubbing against each other, and compressing nerves. On average, the body loses about 1 centimeter in height every ten years after 40.
Risk Factors
Diabetes
Diabetes affects the entire body.
Not keeping blood sugar in check can cause widespread symptoms that affect the nerves and organs.
Individuals with diabetes have an increased risk of developing sciatica and other nerve-damaging disorders.
Genetics
If spinal conditions are part of family medical history, there is an increased risk of developing sciatica.
With chiropractic, elderly individuals can attain better quality sleep, improved mood, and increased energy levels.
A chiropractic physical therapy team can develop a specialized/customized treatment plan for preventive and palliative care.
Body Composition
Sarcopenia
Sarcopenia affects the elderly population’s mortality, cognitive function, and quality of life. As the elderly population is living longer, preservation of lean mass becomes an integral part of maintaining an individual’s independence. Loss of muscle in the arms and legs is linked to decreased mobility, increased risk of falls, and prolonged hospital stays. Falls and fractures often result in a cycle of muscle deterioration. InBody can help track body composition changes and help to minimize muscle wasting and risk of impaired mobility.
References
Aggarwal, Sameer, and Nityanand. “Calcium and vitamin D in postmenopausal women.” Indian journal of endocrinology and metabolism vol. 17,Suppl 3 (2013): S618-20. doi:10.4103/2230-8210.123549
Dougherty, Paul E et al. “The role of chiropractic care in older adults.” Chiropractic & manual therapies vol. 20,1 3. 21 Feb. 2012, doi:10.1186/2045-709X-20-3
Ferreira, Manuela L, and Andrew McLachlan. “The Challenges of Treating Sciatica Pain in Older Adults.” Drugs & aging vol. 33,11 (2016): 779-785. doi:10.1007/s40266-016-0404-z
Kherad, Mehrsa et al. “Risk factors for low back pain and sciatica in elderly men-the MrOS Sweden study.” Age and aging vol. 46,1 (2017): 64-71. doi:10.1093/ageing/afw152
Sciatica motor vehicle crash. After an automobile crash/accident, symptoms of pain and discomfort can immediately follow the force of impact, indicating an injury. Many injuries and symptoms appear right away, like:
Pain from high-impact trauma and cuts.
Bone fractures.
Dislocations.
Neck whiplash.
Back pain.
The sciatic nerve is the largest in the body, and any damage can cause pain in one or both sides of the body. Pressure and compression on the nerves, ligaments, and muscles accompanied by weakness or numbness in the lower back, legs, or feet could cause delayed sciatica symptoms hours, days, even weeks later. It is critical to meet with a doctor and auto accident chiropractor after any type of accident, large or small, to develop a thorough personalized treatment plan.
Sciatica Motor Vehicle Crash
Sciatica can be brought on by a pinched nerve, which is often the result of the spine shifting out of place, causing herniation and compression on the sciatic nerve. The trauma from a motor vehicle accident can cause the spinal discs to be knocked out of place, rupture, and leak out, irritating the surrounding tissue and nerve endings. Back injuries are among the most common forms of damage/injury resulting from a motor vehicle accident/crash that can lead to sciatica. Broken and/or fractured vertebral, hip, or pelvis bone fragments can compress the sciatic nerve. Even when the initial result of the impact does not result in sciatica, over time, an untreated back injury could lead to sciatica symptoms.
Symptoms
Motor vehicle crashes often activate or aggravate pre-existing conditions like asymptomatic degenerative disc disease, affecting the sciatic nerve causing discomfort and pain. Common symptoms include:
Mild discomfort or achiness.
Tingling sensations from the lower back and down the back of the leg.
Weakness, numbness, or difficulty moving the leg and foot.
Inability to bend the foot upward at the ankle- known as foot drop.
Constant pain in one side of the buttocks or leg.
Sharp pain that makes it difficult to stand up and walk
Difficulty sitting.
Burning or tingling in one leg can worsen when sitting.
Intense pain.
Sharp burning and/or what feels like shooting electricity pain.
Diagnosis
A spine doctor and chiropractor will use diagnostic imaging tools like X-rays, and CT scans to see the scope of the injured area.
An X-ray will show a detailed image of the spine and affected bones in the area.
A CT scan will include a 3D image that shows the surrounding musculature, tissues, and nerves that could be damaged/injured.
Treatment
The doctor and chiropractor will then develop an appropriate and personalized treatment plan that could utilize various methods and techniques.
Chiropractic is commonly the first treatment to realign the spine and relieve pressure on the nerve.
A pain management specialist or physical therapist will be brought in for rehabilitation/recovery as adjustments progress.
Orthopedists and neurologists may be brought in for less conservative treatment in more severe cases, including surgical options.
Other treatments can include steroid injections or anti-inflammatory medicines to relieve nerve pressure.
Body Composition
Injury Rehabilitation Phase
Current in-clinic methods of measuring the composition of an injured body are indirect, while medically advanced techniques limit the frequency of testing. InBody provides cost-effective, comprehensive, and timely measurements that identify areas of weakness from damage, injury, or recent surgery and develop a customized rehabilitation program to improve functional status.
During the rehabilitation phase, increased sedentary behavior and/or immobilization causes muscle loss in the injured or operated region. By independently evaluating lean mass in each segment of the arms, legs, and torso, a chiropractor or physical therapist gathers baseline information on the body segments with restricted mobility.
InBody can help provide further insight into an individual’s body composition to analyze long-term health risks and develop a personalized exercise intervention to improve overall health and reduce health risks. This provides beneficial information for identifying potential imbalances related to muscle loss post-injury/surgery that can be targeted and improved. Identifying these imbalances allows the therapists to increase functional fitness and mobility, helping the individual reduce the risk of re-injury or new injuries.
References
Defouilloux, B et al. “A propos de trois observations chez des polytraumatisées de la route présentag une fracture du bassin associée à des signes neurologiques” [Apropos of 3 cases of multiple traffic injuries presenting pelvic fractures associated with neurologic signs]. Journal de radiologie, d’electrologie, et de medecine nucleaire vol. 48,8 (1967): 505-6.
Noble, J et al. “Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries.” The Journal of trauma vol. 45,1 (1998): 116-22. doi:10.1097/00005373-199807000-00025
Walsh, K et al. “Risk of low back pain in people admitted to hospital for traffic accidents and falls.” Journal of epidemiology and community health vol. 46,3 (1992): 231-3. doi:10.1136/jech.46.3.231
Sciatic nerve injury happens from trauma to the nerve and can cause numbness, tingling, loss of muscle power, and pain. The traumatic experience can be a muscle spasm that pulls and/or pinches the sciatic nerve, force/pressure impact injury, over-stretching injury, or a laceration/cutting injury. A slipped disk, or herniated disk, is the most common cause of irritation on the sciatic nerve. A slipped disk occurs when one becomes slightly dislodged, pushing out from the spine. This places pressure/compression on the sciatic nerve.
Trauma to the lower back, buttocks, or leg from an automobile accident, sports injury, work injury.
Medical treatment causes:
Direct surgical trauma.
Total hip replacement surgery can cause nerve compression and stretch during the procedure, causing damage to the sciatic nerve resulting in dysfunction.
Injection injuries via intramuscular injection in the gluteal region. This is a situation where there is a loss of movement and or lack of sensation at the affected lower extremity with or without pain.
Injection palsy can begin suddenly or hours following damage to the sciatic nerve.
A misplaced intramuscular injection at the gluteal region is the most common cause of injury. It is attributed to frequent injections or poor techniques resulting from inadequately trained or unqualified staff.
Complaints of radiating pain in the leg, which follows a sensory nerve pattern.
Pain radiates below the knee, into the foot.
Complaints of low back pain, which is often less severe than leg pain.
Report of electrical, burning, numbing sensations.
Diagnosis
A detailed subjective and objective physical examination is necessary to figure out the severity of the sciatic nerve injury. Diagnostic studies include:
Chiropractic and physical therapy exercises and stretches improve nerve regeneration after nerve damage.
Electrical Muscle Stimulation
TENS and Electroacupuncture have been shown to help enhance nerve regrowth.
Bio-laser stimulation can help with nerve nutrition and regeneration.
Joint or Soft Tissue mobilization
Helps to retain muscle, nerve, and soft tissue flexibility and prevent deformity.
Balance Training
Coordination, strength, and flexibility exercises help to restore balance.
Splinting
In the early stages after a sciatic nerve injury, bracing may be needed to prevent deformity and new injury or re-injury risks.
Ankle Foot Orthosis – AFO can help prevent foot drop, muscle damage, and falls risk.
Body Composition
Optimize Diet for Fat Loss
Individuals that want to lose fat need to create a calorie deficit. Individuals need to consistently eat less than they need for Total Daily Energy Expenditure – TDEE. The safest way to handle a caloric reduction is to reduce calorie intake in small doses like 200-300 calories, for example. After a week or two, perform a body composition analysis. If Fat Mass numbers begin to drop or not, adjust calorie needs accordingly. Restricting calories is the most common way, a deficit can also be created by increasing calorie needs through exercise.
References
Kline, D G et al. “Management and results of sciatic nerve injuries: a 24-year experience.” Journal of neurosurgery vol. 89,1 (1998): 13-23. doi:10.3171/jns.1998.89.1.0013
Schmalzried, TP et al. “Update on nerve palsy associated with total hip replacement.” Clinical Orthopedics and related research,344 (1997): 188-206.
Shim, Ho Yong et al. “Sciatic nerve injury caused by a stretching exercise in a trained dancer.” Annals of rehabilitation medicine vol. 37,6 (2013): 886-90. doi:10.5535/arm.2013.37.6.886
Suszyński, Krzysztof et al. “Physiotherapeutic techniques used in the management of patients with peripheral nerve injuries.” Neural regeneration research vol. 10,11 (2015): 1770-2. doi:10.4103/1673-5374.170299
Sciatica Causes: The sciatic nerve forms by the union of Lumbar4 to Sacral31 nerve roots and exits the pelvis through the greater sciatic foramen, below the piriformis muscle located deep in the buttocks. The nerve runs down the back of the thigh, into the leg, and ends in the foot. The sciatic nerve becomes inflamed, irritated, and/or mechanically compressed. Any type of pain and/or neurological symptom/s from the sciatic nerve is referred to as sciatica. Sciatica is a type of lumbar radiculopathy, which means that the pain originates from the low back and/or sacral nerve roots.
Sciatica Causes
Physical forces on the nerve can cause mechanical compression due to the following conditions:
Herniated Discs
A disc in the lower back can bulge or herniate, causing irritation and/or compression of a sciatic nerve root.
Foraminal Stenosis
Stenosis, the intervertebral opening through which the nerve roots travel, begins to narrow/close in, can compress or irritate the sciatic nerve.
Degeneration
Degenerative changes in the spine like the thickening of facet joint capsules and/or ligaments can compress the sciatic nerve.
Segmental Instability
Instability of a spinal vertebral segment that happens if one vertebra slips over the one beneath it – spondylolisthesis
Complete dislocation of one or more vertebrae can compress the nerve root/s of the nerve.
Other Sciatica Causes
Tumors, cysts, infections, or abscesses in the lower spine or pelvic region can also cause sciatic nerve compression.
Chemical Inflammation
Chemical irritants can include hyaluronic acid and/or fibronectin/protein fragments that leak out of degenerated or herniated discs. These irritants can cause inflammation and/or irritation of the sciatic nerve.
Degenerated discs can cause nerve tissues to grow into the disc, penetrating the outer and inner layers of the disc, causing sciatica. Immune system responses can contribute to pain when exposed to disc fluid.
Substances such as glycosphingolipids/fats and neurofilaments /protein polymers secreted by the immune system are increased in individuals with sciatica. These substances are released from the reaction between nerve roots and exposed disc material, causing inflammation.
Job Occupation
Individuals with specific jobs have an increased risk of developing sciatica. Examples include:
Truck drivers
Desk workers
Teachers
Warehouse workers
Machine workers
Plumbers
Electricians
Carpenters
Fitness trainers
Sitting and standing for long periods, using improper posture, constantly bending, twisting, reaching, and regularly lifting are risk factors for sciatica.
Piriformis Syndrome
Piriformis syndrome is a condition where the piriformis muscle swells and spasms from overuse or inflammation irritating the sciatic nerve that is right underneath. The nerve can get trapped in the muscle causing sciatica-like symptoms that include:
Pain follows the same pattern in the leg as a compressed sciatic nerve root.
Tingling
Numbness
Discomfort from piriformis syndrome feels similar to sciatica, but it is not caused by compressed sciatic nerve root. Piriformis pain comes from compression of the sciatic nerve near the piriformis muscle.
Genetic Sciatica Causes
Sciatica caused by degenerated and/or herniated discs can be genetic. Research has shown that certain genetic factors are more prevalent in individuals with back and spinal problems. These congenital disabilities can cause the discs to become weak and susceptible to external stress. With time the proteins in the disc break down, compromising the integrity and function.
Arthritis and Joint Issues
Arthritis or other inflammatory conditions around the hip joint can cause pain down the leg, similar to sciatica. This is referred pain that spreads out from the source and is not radicular nerve pain that originates in the nerve roots.
Conditions like sacroiliac joint dysfunction or sacroiliitiscan cause sciatica-like pain that runs down the back of the thigh but usually ends before or at the knee.
The pain can be acute and debilitating, like sciatica but is caused by an abnormal motion or malalignment of the sacroiliac joint.
Body Composition
Normal Cholesterol Ranges
High cholesterol can lead to severe consequences when left untreated, but it can be difficult to spot with no noticeable warning signs. This is why it’s essential to monitor cholesterol levels with blood tests, especially if there is an increased risk. Example of normal cholesterol levels for adults 20 years of age or older:
Total cholesterol 125-200 mg/dL
LDL <100 mg/dL
HDL >40 mg/dL men, >50 mg/dL women
Lifestyle
Lack of physical activity contributes to high cholesterol levels.
Diets that mainly consist of processed foods and saturated fats increase the risk of high LDL levels.
Smoking can lower HDL levels.
Aging
Individual risk for developing high cholesterol tends to increase as the body advances in age. This is why it is recommended to have regular physicals and blood tests.
Genetics
Some individuals are more genetically predisposed to developing high cholesterol and heart disease.
Knowing family medical history can help predict whether it may become a problem.
References
Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2021 Sep 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK507908/
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK482431/
Hicks BL, Lam JC, Varacallo M. Piriformis Syndrome. [Updated 2021 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448172/
Raj MA, Ampat G, Varacallo M. Sacroiliac Joint Pain. [Updated 2021 Aug 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK470299/
In today’s podcast, Dr. Alex Jimenez, health coach Kenna Vaughn, Truide Torres, biochemist Alexander Jimenez, and Astrid Ornelas, discuss how chiropractic care can ultimately help treat sciatica or sciatic nerve pain.
Dr. Alex Jimenez DC*: Hey, guys, we’re live today. We’re going to be discussing the scourge of the back, the scourge of the back for myself. I’m a chiropractor practicing out here in El Paso, Texas. We usually have a disorder that’s typically there isn’t a day that we don’t see it, and it affects so many people. But there’s a lot of confusion with, and I call it, the scourge of the low back. It’s called sciatica. Sciatica is a disorder that has many, many reasons and many, many causes. One of the most important things is first to assess the reason and cause of sciatica. But most importantly, when it first hits an individual, it strikes them, usually with a shocking misunderstanding as to what’s going on in their legs. They feel pain in the low back. They sometimes feel pain in the leg. Different areas depend on where the issue lies, so a little bit of its anatomy breakdown and explanation of what it is. First of all, it’s a syndrome. It’s a syndrome that has many reasons and many causes. The issues that come about and are that that make sciatica arise are vast. I would venture to say that there are a million people that come in with sciatica. There are a million reasons that have presented each one of those patients. There is a majority of problems in and a subset of issues. We’re going to go over that. Today, our goal is to bring out the awareness that it is a problem, just like the present anemia. And there are many reasons why a person would have anemia. Many people are familiar with anemia, and they say that’s low blood, but you’re going to find out where the blood issue is to determine exactly what the causes of anemia are. Well, the same thing with sciatica. There’s a lot of reasons why the sciatic presentation occurs. So we’re here to kind of begin the process of explaining that. So we’re going to get real deep and down and nasty with the science of it. We’re going to try to give you some tools that you can look at and assess. So your provider can give you a better explanation, or you can ask better questions in terms of where your sciatica originates. So the first thing is to understand the anatomy, and I’ll go through the anatomy in a very visual way. But I want to first kind of take you to a visual, and my visuals are very three-dimensional and offered through complete anatomy. Complete anatomy has given us the ability to use this and show, and it is something that many medical students use. So in today’s modern-day, we don’t have to use some visceral or some sort of human anatomy. We can use these tools to help us present to the patients and to teach. So it’s probably one of the most used anatomical structured systems, and we use it to teach people in our patients every day, given the dynamics of sciatica. Here we have a picture of a sciatica HDMI, so we can see a presentation of what the sciatica nerve looks like when we can see it. The interesting dynamics here is that when you look at the interesting presentation, you can see as I go away how vast and how large it is. Now the first thing is I rotate this individual. You got to see that it comes from a large glute plexus in the lumbar spine to the sacral nerve roots. So anywhere down the line that anything is touching this thing, this beautiful, powerful nerve, you’re going to find that there is pain radiating down. So we’re going to discuss those issues. And as we kind of go over that, we want to understand that so away from HDMI. So what we’re looking at are the issues that present with us when we discuss it. So what are the causes, and what is sciatica? Sciatica is inflammation of the sciatic nerve, and as it presents what happens many times, it is the largest nerve in the body, and it’s how most people know it, and it travels from the lumbar plexus to the leg. So, anywhere that that thing is touched, it’s going to radiate pain. Now, what are the causes? Well, they could be from vascular. They could be compressive. They could be lymphatic. There could be a space-occupying lesion, such as a tumor causing the issues. Now, a good clinician will do a lot of different tests and a lot of different assessments to determine where it is having the problem. So when I have a patient, they come in when the first thing we have to do is a history we have to assess and find out what’s going on. So finding the history of something that suddenly someone starts sitting or they become active, or they get hit in the back, and they start having sciatica, it boats to a well, dynamics. So what happens is, what we need to do is we need to discuss the dynamics of where it begins and what goes on. So in terms of our direction, I would like first to take you to the physical assessment. When you explain to your doctor what’s going on, you need to tell him exactly when you started having it. That’s very important. The history is very like when these issues are? Do you have a sedentary life? So these are the types of issues that present most of the time a person comes into the office with having a severe presentation that they’re shocked? They didn’t expect this and what occurs in this particular area is that you can see where the nerve root comes in. So over here, you’ve got to figure out where it came from. As you notice, a lot of the reasons that many of these individuals have is because it’s a little bit of atrophy and muscular issues that arise. As you can see right here, there’s a lot of areas where the nerve can keep becoming trapped, and this is the main reason that most people have this issue now as they go through this and they present a symptom. I got to figure out, and we have to figure out where the problem originated with our team. So as I go through that, I want to give you a different dynamics here in what I’m going to explain. I’m going to present my team to you so that they’re all going to. Each one of them is going to explain a little different aspect of what goes on. Today, we will discuss how a coach, such as an individual helping the doctor, can assess the situation. We are going to talk to our coach Kenna. We’re going to talk to Astrid, who’s going to bring some science knowledge here. We will bring a patient in, discuss the experience with her, and bring in our top guy from the university at the biochemical level. He will teach us a little bit about some nutraceuticals and some applicational processes that we can do to help an individual with sciatica. So at first light to tell, I like to ask a question to Kenna. So Kenna, what I want to do is I want to ask you exactly what it is that you notice when a patient presents with sciatica and what kind of things we can do in the office and what’s our approach specifically more like the metabolic issues and the disorders that present that way? So when we’re looking at here, let me go ahead and head into this area, tell me a little bit about how we present a patient and what we deal with when we’re talking to an assessment or doing an assessment.
Kenna Vaughn: So one thing that many patients with sciatica have is the pain they’re feeling, of course and that low back. But another thing is they don’t have a lot of movement due to that pain, and movement is essential. It’s what life revolves around. So we take that movement, and we look at how we can help this patient decompress that sciatic nerve with the adjustments that Dr. Jimenez does, but also how can I benefit from my side of things for this patient? So we do have a lot of great resources available to us. We send our patients to Push, which is a gym here that helps them get that calibration in their muscles that they need to build up those stronger muscles all around that sciatic nerve so that this nerve doesn’t get pinched frequently or as often. And another thing we have available to us is an app called Dr. J. Today. And what that does is it syncs with the bracelet that our patients wear, which allows us to track their movement. So we want to focus on that movement as part of it. And another thing we can do is nutraceuticals in supplements. So what are nutraceuticals and supplements? One of the main ones we focus on that almost every individual should be taking is vitamin D3, and we like it coupled with vitamin K. This will help your bones and circulation. And it’s going to help to decrease that glucose by increasing your insulin sensitivity. And this is where it comes into play with sciatica.
Dr. Alex Jimenez DC*: I had a question for you in terms of that. When you’re discussing that we’re dealing with and sciatica as a pain in the hips, we’re correlating, and we’re tying together, I guess, a disorder that many people have as metabolic syndrome and many times are overweight. And that was one of the presentations that many of the patients with sciatica, not that everyone is overweight, with sciatica. Still, many people who become sedentary and don’t move as much do suffer from metabolic syndrome. So to get that under order, one of the things is to bring the insulin under control. And once we do that, we start losing weight and getting more active with the exercise protocols. She mentioned Push because we began to calibrate the hips. Now, as you can tell from our picture here, there’s a whole lot of muscles in this region, OK? So as I kind of use the application, you can see a little bit more of the muscle tissue that is involved. So as we look at the muscle tissue, we can see that calibrating and these muscles that control the hip actually propel the creature, so propel humans, so to speak, right? So what happens is as this happens, if this becomes deconditioned through a sedentary lifestyle. Well, the thing that’s lying underneath also stops working, and the muscles stop working as effectively. So one of the ways that we treat people is through a coach to assess their body mechanics and put them through the Push Fitness protocols that can help them get a calibration of the structures. One of the things that we also do in this process is we look at the sitting issues and tell me a bit of what you do, Kenna, in terms of helping people adjust their lifestyle or modify their mobility issues.
Kenna Vaughn: So what their mobility, as I said, we use the app, and we also use Push Fitness, and the supplements have a lot that comes into play because like I said, with that increasing the insulin sensitivity, what we’re going to want to do it, that is it’s going to help to control the blood sugars. And you might not necessarily relate blood sugars to sciatica just yet, but as I said, everything is connected. So when we put our patients on a protocol and have them control these blood sugars, it also helps maintain their inflammation because sugars and chemicals cause that inflammation in the blood. And that’s also it’s going then to cause nerve damage to our body and our system. And then, once we have that nerve damage going, we’ll see many more patients sitting down, which relates to that lack of motion. And then we see a lot of patients coming in with sciatica.
Dr. Alex Jimenez DC*: Sciatica. So basically, we’re going back to the same monster, which is called inflammation. Right. So inflammation is the deal. People that have sciatica will often tell the story of how it kind of looms with them. It’s like having this untrustworthy nerve back there that if they have stress or go through emotional dynamics, it affects sciatica. So this threshold that activates the sciatica presentation could have even an emotional component to it. So we want to bring that to light, too, because many people have normal lives, but they don’t have the presentation under normal situations. Suddenly, bam, they get an emotional, financial issue, family things, and sciatica just flares. Where is that even logical, right? The key is inflammation, inflammatory response, stress responses. And those issues do create an almost perfect storm to create a predisposition for inflammation. So that’s why we bring in the dietary components and the food to start eating better to prevent inflammation again. Those are some of the things. So she also mentioned the issue of Push. Push is our fitness center, where we actually put people through exercise protocols, and when we start putting people through exercise protocols, it’s there to calibrate. Now, what’s the biggest muscle in the body? Well, not too far from the anatomy to an anatomical structure. You can see the muscles in this particular area, and everybody knows that the glutes are the big muscles. So when you see this powerful muscle, if this muscle becomes decalibrated from a sedentary lifestyle, you’re going to notice that you’re going to have a lot of predisposition. So it’s like a car with flat tires. So if the car has flat tires, it starts swaying and moving to the wrong side. Well, if it’s swing, you can imagine that it affects the axis and the axles, and all that kind of stuff starts happening. Things like these happen, but in our human structure, there’s a finely calibrated system here. One of the things that many people don’t know and don’t think about is the lymphatic structure. Now, if you can see here, you can see the lymphatic. Now those guys ride directly next to the venous and arterial structures, and you can see it here. So as you can see that for progressing, you also look at the arteries. So if someone doesn’t have an arterial system that is working well and sitting on this, you can see congestion occurring around the structures, around the nerves. Now there’s a lot of nerves in here. So when you start looking at these dynamics, you start seeing that a person who is not using their muscles has an increased congestion level. So as I remove these muscles here, you can see this picture, and I’m going to remove every one of them. You start seeing the noticeable dynamics of how complex their nervous system is. So over here, you can see the complexity of how those nerves function. It’s amazing to see all the structures in here. So when you look at this, you can see the amount of influence that lack of movement would cause. It’s almost like a traffic jam. Imagine sitting on this thing all day long, OK, let alone be inactive. So one of the things we want to do is to assess exactly what it is. And one of the things that we do is to calibrate the system. So going back to removing these picked areas, you want to go ahead and work on the big systems. OK, well, as you can see, these muscles bring a huge component into helping sciatica. Now, where are the sciatic issues coming from? Now let’s go ahead and start discussing those particular issues as we can kind of go through this. And I want to take you through a little anatomy lesson here because it does require a little bit. As I remove these things, we’re going to see all of the structures that come in, and actually, but you can see if I can get the nervous system only out to the minimal component of it, the big ones. And as you can see here, you can look over this way and see anywhere down the line right here by where the nerves are. Them out where the disk comes out in this particular area as it penetrates forward, it goes this what we call the sacral notch, which is this guy right here. This hole is a sacral notch where it comes out, and you can see that it can be bumped into the bone and the actual femur here. So there’s a lot of areas that we can see that directly affect the sciatica regions. But having gone through that, I’m going to go into that in a little bit deeper. But I want to go ahead and get a little personal story right now. I want to ask an individual now what sits in here, and most women, you know, this is where they contain babies, right? So in a situation where you have an individual that is going through a lot of changes, such as an individual who’s having a child, you can see where the hips actually change and right down there, if you can see down there, this is where the sacrum has to open up to allow for the birthing canal. You see that big hole right there. A baby’s got to go through there, and if it can’t go through there, which it probably won’t until probably the ninth month where this area starts expanding, guess who’s going to go by, then kick in on the way down? OK, that would be a child. OK, so let’s talk about that. I’d like to present Trudy here because she has a story of how it affected her.
Trudy Torres: Well, I guess, you know, as a woman, you know, it’s an extremely joyful situation when you find out that you’re going to be a mom. If it’s your first-time baby, you’re in for a roller coaster. You know, like you guys were mentioning, there’s a lot of different scenarios that you go through emotionally, physically. So when you’re pregnant, you’re the perfect storm for something like this to come up. You know, you are just balanced from you’re so, so tired the first trimester. I’ve always worked out. So for me, I have never experienced sciatic pain before, and for me being so active, I went from being 100 percent active to just being so tired. I had to be super careful about spending my energy, especially in the first trimester. So on top of that, if you add, you know, everything else that’s going on physiologically with me and then my life became so sedentary. On top of that, you know, I have a desk job. So sitting at a desk and then not compensating, moving all of a sudden, that pain is so excruciating. I did not experience this with my first baby. I experienced this with my second child. And, of course, I gained more weight with my second child. So once again, you know, you’re adding problem over the problem. And just because you’re pregnant, that doesn’t mean you’re eating for two, because unfortunately, some of us, you know, have that misconception, and that’s when your weight tends to get a little bit out of control. So you’re adding a lot of different factors that create the perfect storm and are just super, super hard. One of the things that Kenna mentioned that helped me was becoming active and being exposed to Push. I had someone here that was able to work out specifically with me being pregnant. Obviously, my limitations as you start gaining more weight, it’s not the same thing that you can do when you’re not having a baby. So I was able to continue to work out later on in and, you know, after I was exposed to chiropractic and implementing exercise.
Kenna Vaughn: So the main symptoms you had when you had sciatica, and you were pregnant, was it mainly just pain, or did you also get that tingling feeling because there is more than one symptom of sciatica?
Trudy Torres: No. Unfortunately, it was just not pain. It was pain. It was burning all down my leg. I did not know what was going on. As I said, this was not with my first pregnancy, and every pregnancy is different with my first child. I watched more what I ate. I was still active, so I believe it was a combination of things, you know, that I felt like I was eating for two. I gained more weight than I should have.
Dr. Alex Jimenez DC*: I got a question: Was it when you rapidly gained weight during the final trimester?
Trudy Torres: I think everything kind of started happening a little at a time. I wasn’t that active in the first trimester, so I began having flare-ups not as bad as once I gained the weight. But, you know, once I gained more weight, that’s when I started having more severe symptoms, as I said, the burning, the lower pain. It was just excruciating, and it’s something that I don’t wish upon my worst enemy.
Dr. Alex Jimenez DC*: Now, did you ever have a recurrence after you had your baby?
Trudy Torres: Yes, I did. I did, and unfortunately, I did, but one of the things has helped me keep that under control. It’s been being active, continue to watch my weight. My supplements were one thing that I would ask Coach or Dr. Jiménez when you’re pregnant. I know we were talking about the different supplements. What do you still recommend for pregnant women to get on the different vitamin D and K supplements?
Dr. Alex Jimenez DC*: That’s an excellent question, and one that I’ll answer very clearly as a wide disclaimer; you need to make sure that your doctor knows what you’re experiencing. Obstetricians, which are OB-GYN doctors. They’re very well astute as to what type of supplements. So in the world of supplementation, it is wise to have a doctor assess that, and many of them will make sure that you have good supplementation. The area where it’s the accurate assessment is you have to have supplementation. Your body’s trying to produce an enormous amount of cellular activity as it creates life. It draws upon a particular area that inflammation goes crazy, the body goes into dynamic changes. So nutrition becomes an essential thing from intestinal nutrition through metabolic nutrition. So one of the things is that you have to have a doctor, typically today’s individual who is in there as young childbearing age, they have a doctor evaluating. So yes, one of the essential things is from folic acid to vitamin E, D. These are a whole, complete gamut of vitamins that are assessed and given by their doctors. So most women will know that if they take some medication, they have to put it clearly by their doctor. That’s the most important thing. And the second thing is on the supplementation side; once your doctor knows, he’s probably going to give you something of a basic level of supplementation and nutritional assessment. So in terms of that, a dietitian can evaluate you and assess you and determine what’s going on in terms of the aggressive approaches where an individual is not pregnant; there’s a lot of things that can be done. But let me ask you this. I know that you do a little bit of a CrossFit, and you do that kind of stuff. And you mentioned that you had sciatica after. I want to go to the point that many people who have sciatica lead a predisposed life to sciatica now, meaning that once you get it, it’s not that your terminal is that you always have the potential of having it, so whether your body dynamics have changed. Typically, you’re not 18, and now you’re 40. What happens is your body is warning you that it’s not working as it should be. And suddenly, the nerve starts becoming flared up, either the compression through atrophy of muscle or imbalance of muscles. So all those things are essential; I notice that you mentioned something that you did. It also affected you after. Did you do some competitions later, and did it affect you?
Trudy Torres: I did do competitions after. What helped me keep it under control was that its different factors to keep it under control. You know that keeping moving makes sure that you’re taking the right supplements in chiropractic care. I’m a firm believer, you know, of a holistic approach, and I believe that a combination of all it has helped me keep it under control. I have not had flare-ups, but I believe it’s because I’ve had all these different combinations. As I said, you know, I kept active. I have, you know, been in average weight. I have also implemented chiropractic, you know, as maintenance.
Dr. Alex Jimenez DC*: You know, I would like to give people a kind of insight as to what happens when you first go to a doctor, and they assess you; there are many ways to figure it out. One of the ways that it’s an easy way if there’s degenerative and there are bone changes is an x-ray. And that’s what we typically look at, and we first start all assessments. But the definitive assessor who gives the vast amount of information is looking for some compression. And at that point, sometimes we have to look at the arterial-venous circulation. But the number one way to determine if someone has sciatica due to a disc injury or some compression or space-occupying lesions like a tumor or some arthritis or some sort of imbalance in the muscle is genuinely the MRI. The MRI is an excellent tool. Now, if there is bone involved, a CAT scan is used. The EMG is used to determine the muscular tone and the muscle’s ability to react and see which tone levels. But you don’t need to be a rocket scientist and put someone through that. They already know that their muscles are tight, and there is an issue. The ability to determine how the nerve functions is a nerve conduction velocity test that tells you how fast and slow the nerves could work. Now in the situation where we do a bone scan, we’re trying to look for any metabolic issues outside, and there could be a tumor or some problem. But that’s rare, and that’s not typical, but the number one way to assess an issue is through an MRI and an X-ray. Those will give you the most significant, broadest areas. Now I want to go ahead and talk a bit about nutraceuticals and specifically nutraceuticals. We’re going to go ahead in this about the treatments for it. And as we go through that, I’d like to go ahead and discuss certain areas and specific supplements. Now Astrid is our resident nutraceutical information gathering. We also have a biochemist in the background who will bring some insight to a different level. But what kind of things do we typically offer patients when they need it as a metabolic, a leaving protocol?
Astrid Ornelas: OK, well, first of all, I want to bring in an interesting statistic. According to researchers, approximately 80 percent of the population suffer from some type of back pain. Included in that are low back pain and sciatica. So with that being said, of course, it becomes a priority to know what is it and what can we do to assess this common problem? And like, Kenna and Dr. Jimenez, like you and Trudy have said, exercise is essential. And together with exercise, we want to bring in a diet. We want to eat foods and supplements. And because obesity or excess weight is one of the problems is one of the leading causes or one of the most common, commonly well-known causes of sciatica. We want to, you know, all together with exercise and following like a good, a good diet. We want to follow these things so that we can. If we lose weight, it can help improve sciatica. So with that in mind, there are several of them. I guess natural remedies, natural nutraceuticals, if you will, can help reduce or improve sciatica symptoms and, therefore, lose weight. So one of the ones that I want to talk about is that we have it here: turmeric or curcumin. So turmeric is a plant, it’s a flowering plant, and it’s related to ginger. And we eat the root. That’s what we know it. This yellow kind of orange-looking root is very commonly used in Asian foods and most commonly in curry and curcumin. You’ll hear turmeric and curcumin used a lot interchangeably together, and curcumin is the active ingredient that’s found in turmeric. So one of the things that I wanted to bring up with turmeric and curcumin is the benefits that many people can take, and they can either eat turmeric or take turmeric supplements. It can help to reduce sciatica or sciatic nerve pain. So turmeric has a lot of anti-inflammatory properties, which can help reduce pain and swelling, which is probably one of the most common symptoms of sciatica. There’s a lot of research studies that have found that turmeric or curcumin can reduce neural inflammation, which is inflammation in the nerves, which, as some of us here, know if your sciatica is caused by a disc herniation or a herniated disc, sometimes the substances or the chemicals that are inside of your disc, they can irritate the nerves. So taking turmeric and curcumin can help reduce the inflammation caused by these irritating compounds. It is also a powerful antioxidant that can help reduce oxidative stress, which can cause inflammation. And probably one of the highlights of taking turmeric or curcumin is that it can improve metabolic syndrome, as we previously discussed in a past podcast. Research studies have found that turmeric can help regulate body fat by reducing inflammation. It can also help lower bad cholesterol. It can lower triglycerides. It can improve blood sugar levels. And it has antibacterial properties as well.
Dr. Alex Jimenez DC*: Let me ask you. We’re talking about the potential of someone having sciatica; since some people have sciatica, that kind of looms on them. Well, we’re trying to do with turmeric, and we’re trying to prevent it from kicking off. So it’s basically like prophylactic prevention. I like to go a little deeper, and we have our resident scientist here, Alexander, and he is right with us right now, and he’s got some points of view on some of those supplementations. Tell us a bit of what you learned in terms of supplementation and your point of view on how we can assist sciatica from a biochemical point of view.
Alexander Isaiah: Well, there are a couple of different ways of taking different perspectives and avoiding the whole. An inflammation response is a good way of saying it. Let me see. Can you guys see my screen here?
Dr. Alex Jimenez DC*: Yes, we see you, we see you right now. So I saw your screen. Yes, I do. We see the screen entirely.
Alexander Isaiah: Awesome. So I’m going to go into a little bit of the biomechanics of what’s going on with sciatica. Then we’re going to break down a little bit of the muscles, and then we’ll go into the supplementation aspect of what we can do to have either prevention or active treatment during treating sciatica. So here we could see we have three individuals from left to right. The first one is an individual who has a neutral spine. And you can see that as we draw a line down the middle there. External auditory Matis, the ear, is in line with their deltoid and is in line with the median part of the sacrum. In the second person, we can see that they have a little bit of dysfunction in terms of their physical aspect. So here we have an individual whose sacral promontory, which is the anterior side of the sacrum, is tilted superior, and their posterior area is tilted, posterior, inferior. I’m sorry. And what this is called, this is called a counter mutation. So by having that sacrum pointed up, you’re putting more stress on the thoracic region and causing the areas to be more inclined to different stresses. And most of the time, this is caused by tight hamstrings. So these hamstrings are pulling down, forcing the anterior side to come up and stretching these quadriceps. So it can either be done from an imbalance of over-powerful hamstrings or tight hamstrings and weak quads. In the third individual as we draw the same line down the middle. We can see that they are almost in line, but on an individual like this, we could see that their sacral promontory, the front side of the sacrum, is tilted anteriorly, which is called mutations. So we have a counter mutation over here. It’s going to go counter. And then mutation over here on the right side, so an easy way to remember this. They’ll stick forever is that this is pretty much if you think plumber’s butt, this is what it looks like. This is what J-Lo looks like. Oh, so you’ll never forget it that way. But the difference is here is that here the pressure is on the thoracic spine. But in an individual with notated hips, the pressure is in the lower back. So let’s say someone is pregnant and developing another child in this area. They’re going to be putting more pressure on the lower back versus someone who has pressure on their thoracic area. They’re going to be more pressure there. So going into a little bit more of the anatomy. We can see that we have all the different muscles here, and we could see the piriformis, which is this muscle right here. I’m going to give you different colors for you guys, so that you can see better. It is muscle right here. And then we could see the superior gemellus is right under that. So sandwiched between the two is the sciatic nerve. And if we have someone who is mutated, they’re going to be stretching these muscles more and putting more compression on that sciatic nerve, causing that area to be more inflamed. More of those neuropathies are occurring, shooting down the leg. And then in other instances, when we have the piriformis, which is split in half and the sciatic nerve is running between them, and that’s 10 percent of the population that that usually happens. And so and these people have always had sciatic problems. So by strengthening and working on those conditions and going over those nutraceuticals, we’re about to go into, we can treat and alleviate some of those symptoms. So the first one I kind of want to go into is a little bit of niacin. So niacin, we all see it as the store brand as something popping up like that. And most of the time, it’s either in 250 mg or 500 mg of capsules or tablets. I always recommend getting the tablets just because you can take half of the tablets. And I tell people this is because most of the time, nicotinic acid is the main thing is, vitamin B3 causes a little bit of a flush effect, but that’s just the way it works. So we’re going into it here. We can see that nicotinic acid, as it’s going through its chemical pathway, actually produces lots of NAD+, and NAD+ is essential in the cellular metabolism of many tissues. So going into brief biology, we all know that the mitochondria are the powerhouse of the cells we were all beaten to death growing up in basic biology. But as we take a look more in-depth at the structure of the mitochondria, we could see that it has an outer membrane, an inner membrane, and then an interim membrane space. So we’re going to look mainly at this little section here that’s folded in between, which are called the cristae. And we could see that the first complex, known as complex one or all the known as any dehydrogenase, is responsible for using NADH, converting it and using its protons, and moving it across the gradient to make ATP. But we could see that more NAD+ is produced here, right? So that’s where niacin comes into effect. We supplement more with NAD+ to cause a reduction reaction between NADH and some other electrons, forcing it into NADH. So what does this all mean? Pretty much what we’re doing is we’re creating a boulder downhill effect, so we’re making more NAD, and we’re forcing it to go to product. And how does this happen? Just easy thermodynamics is you put a lot of it up the hill. The enzymes are going to force the work to go down the hill and make more energy. In doing so, and you have a more healthy metabolism of cells. And this does not only correlate to neuropathies, but it also helps with circulatory function, cardiovascular health; the main multi nucleotide muscle in the body is the heart, so you’re not only making sure that you’re neuropathies are covered, but as well as you’re making sure that you’re keeping a healthy heart just by supplementing with vitamin B3. Another great one, saying that you have more ATP produced and more functioning and healthy tissues, is green tea. I chose to use green tea because it has a very similar pathway to curcumin in the sense of anti-inflammatory effects. So the main ingredient in green tea in case you either have green tea in your house or curcumin available, whichever one’s easiest for you, they mostly have the same chemical pathways in that they inhibit either inflammation or cell proliferation neural damage. So the main chemical in green teas is called catechins, and catechins are similar to catecholamines, like epinephrine and norepinephrine, which is just adrenaline. And the main one is EGCG. The cool part about EGCG is that it inhibited NF Kappa B and ROS. ROS is just a reactive oxygen species, which is just free radicals, which can cause havoc and wreak havoc throughout your body, which is why it’s an antioxidant. So in doing so, it prevents NF Kappa B from producing any proliferating effects from cells or inflammation or neural damage. Now, if we go more into biochemistry, I can just break it down a little bit here. So EGCG will upregulate AMP. High levels of AMP will down-regulate this enzyme, called glycolysis, and allow for ATP to be converted to CATP. This is important because not only does the CATP break down things, but it mainly breaks down any adipose tissue and helps kill any cells that are proliferating too quickly, such as cancer cells. And it also keeps cells functioning properly, such as neural cells. So as we’re coming here, another cool part about green tea is it has small amounts of caffeine. If you are pregnant, we don’t recommend that you do any caffeine or stimulatory effects. Always consult with your doctor before taking any of these things. Specifically, something that does have caffeine and that we just doesn’t want to mix anything, especially during pregnancy. But if you are trying to make sure that you help your sciatica or your metabolic syndrome. Green tea has another effect. Using caffeine, which inhibits phosphodiesterase and phosphodiesterase diseases, is responsible for turning off CATP, so it’s a double whammy effect. Not only are you burning fat and shutting down glucose storage, but you’re also allowing for this catabolic or this structure that breaks down things to keep going. Here’s a little bit of an overview of the different things that green tea does and how it helps. And just kind of going into another cool part about green tea is that it binds to other very toxic things, such as iron. We know that we have iron in every red blood cell, but people who have hemochromatosis have too much iron in their blood, and they have to give blood about once a week. Someone who has hemochromatosis can take supplementation of green tea and reduce their iron levels, preventing any toxicity from those iron.
Dr. Alex Jimenez DC*: You know, when you’re talking about those pathway patterns, you remind me very clearly that many of the times, the whole idea behind our show is to try to give you natural ways. However, there are potent medications that work with these pathways, one of which is gabapentin, used for neuropathic pain. Many people don’t want to do that because of the side effects and the critical issues that it causes. We were looking at this in a natural format in a natural way. Going back to the metabolic, what are the things that we notice in the metabolic areas you have seen? What are the other supplements? Do you notice that I have been able to assist people in recovering from because Astrid mentioned turmeric, and that’s the line we’re using. We’re using the anti-inflammatory. They’re limiting, limiting the reactive oxygen species or the ROSs to prevent the inflammation from occurring. Is that correct?
Alexander Isaiah: Yes. OK. The main thing is to inhibit the production of NF kappaB, which both curcumin, other known as turmeric, both have the same name. They’re interchangeable and green tea, and both inhibit these inflammatory pathways and cancer pathways.
Dr. Alex Jimenez DC*: Yes. So let me ask you, Astrid, in terms of those inflammatory comments. Tell me a few of your thoughts on this particular matter.
Astrid Ornelas: Well, I wanted to add another compound that can benefit sciatica or sciatic nerve pain. And that is called alpha-lipoic acid or ALA. And so ALA is an organic compound, and it is produced naturally in the body, but of course, in smaller amounts. Or it can be found in foods such as red meat or organic meats or in plant foods such as broccoli, spinach, Brussel sprouts, and tomatoes. Or it can also be taken as a dietary supplement. And I wanted to discuss the effects or the benefits of alpha-lipoic acid. Because just like green tea and turmeric or curcumin, ALA is also a powerful antioxidant, and it helps reduce inflammation, according to several research studies. And it can also have a lot of benefits for people with metabolic syndrome because it can help lower blood sugar or blood glucose levels. It can improve insulin resistance, which is, you know, an effect, or it’s something that they can that can ultimately cause diabetes. And several research studies have also found that alpha-lipoic acid can also improve nerve function, which, you know, people with sciatica or sciatic nerve pain, especially caused by neuroinflammation. ALA can also help improve nerve function in these people.
Dr. Alex Jimenez DC*: OK. That’s an essential point of view. As you can see here on our list, we have quite a few different presentations and areas such as vitamin C, vitamin D, calcium, fish oils, omega 3s with EPA, berberine, glucosamine, chondroitin, alpha-lipoic acid, acetyl-l-carnitine, ashwagandha, soluble fibers, vitamin E, green tea, and turmeric. As you can tell, there’s a lot of things that we can do to stop the inflammatory cascade. We’re going to be going into all those because sciatica is so complex and diverse that we have to find the best for the patient from the millions of presentations that it has. So throughout the anatomy, as we discussed, and I’ll show you back the anatomy in a second here, you can see that there’s a lot of physiological and as Alex presented biomechanical imbalances that, if not taken into consideration, we will end up with issues in the future as a result of these predisposing dynamics. Now, as we recover these dynamics, we’re going to discuss many different topics. So I wanted to at least give a little more on the side of the things that we do now in terms of differential diagnosis. Many other issues can cause these presentations and from, you know, the dynamics of just a compressive nerve through space-occupying dynamics. We have other areas that come in and affect the patients. So what we’re going to do is in the following seminars, we’re going to go over specific types of things we can do, but let’s give you some guided ideas in terms of the treatment protocols that are out there. We have chiropractic care, which is a form of chiropractic. Chiropractic means mobilizing joints and moving the body, and there are thousands of ways we can do it. A lot of people think that it’s just manipulation or adjusting the spinal. We have to take a lot of things into consideration. We work on the bones; we work in the muscles; we work on the counter muscles. We have to formulate many dynamics to figure out what’s best in line to assist each patient. Once we find out the cause and find out what we call etiology or the pathology and the problem. We can go and use different methods. We use acupuncture, nutraceuticals. We work hand in hand with different providers to provide medications. We also do the goal ultimately in sciatica is to eliminate any chance of surgery if there is a surgical need or that needs to be done. But that’s such a small dynamic that we don’t want to go there unless we have to. We have different other protocols in different methods of treatment, like dry needling. We do aggressive rehabilitation. Now, why are we doing rehabilitation? Because as you saw in the picture earlier, the muscles we have were extremely involved in calibrating the hips. We want to make sure that we, we determine now over here, we got some basic care. We also got some aggressive care. Now, as you know, some basic care will be like ice-cold ultrasound, tens units, spinal adjustments, lifestyle changes, which is pretty much the biggest one because most people end up in a chiropractic office because their lifetime lifestyles change. Now, what do I have? I have a person who was an athlete at one point that suddenly got a desk job and now doesn’t move as much. Well, that’s easy. We can start getting that person back into yoga, pilates, tai chi, getting their bodies to align pelvically, and their whole body structure to get back to where it should be. Here’s the deal as soon as you can get past the inflammation and prevent that, and we can get you to move your body in a way that you did when you were a child, kind of like moving, dancing, and walking. That’s the way to calibrate the glutes. This is a powerful muscle, and as we’ve learned through technology and science, immediate atrophy occurs with the muscles not used. So imagine what happens when you start getting a job, and you used to be an athlete, and now you sit down eight hours a day, that’s going to give some great dynamic. So one of the crazy components is that as I look at this, I give you an idea of the types of exercises we can do. We can go into the extreme kind of CrossFit environment. And if we look at that, you just don’t look at the crazy structures, but you see people moving dynamically. A lot is going on here, and you can see that we can come up with our rehab centers. We have extreme athletes, too, even the people that are, you know, able to move just a little bit. But the point is that as we do this process, we can help someone with the treatments and protocols occurring, as you can see in this particular area. We can see Trudy and me. This is one of the things that the reason I was alluding to. But we can see when you were doing some self-treatment here. Tell me a little bit about what you were doing and what you were experiencing at that point.
Trudy Torres: That was, I believe, if I recall correctly, that was after my competition. I did compete for CrossFit. And, you know, it’s hard, after for a couple of hours. It takes a toll on your body. So I was kind of stretching my hip and stretching, you know, the rest of my glute area to avoid that flare up again. That’s something that once you experience it once and you have to go through the treatment, it stays in the back of your head because you certainly don’t experience pain again. That’s why you have to pay attention to all the different preventive areas and approaches to avoid ever having a flare-up.
Dr. Alex Jimenez DC*: Well, I got to tell you that I led you there because I know you had a lot of experience with sciatica. Alex, let me ask you this. You know, you were an aggressive competitor in the world that you did things. Tell me a bit of the thing that you did that you noticed when you were working. Let’s say an as a collegiate athlete, did you ever have hip issues?
Alexander Isaiah: Only when I didn’t stretch or when I didn’t work on my core muscles, or when I wasn’t making sure that I was anatomically in line, I did have some issues either with joint pain or just lower back problems or even upper back problems that all just tied into either flexibility or I just wasn’t paying attention to either my diet as strictly as I should, especially at that level. So, yes, I did.
Dr. Alex Jimenez DC*: Yeah. You know what? There’s a lot to be covered here, and we’re going to be discussing a lot of issues. Did anyone want to add something else before we kind of closeout? I want to thank my crew for what we’ve done here. We are going to continue with this. Because we’re going to go real deep, this story of sciatica is going to get nasty with information. This is the beginning of touching on the subject matter. Thank you, Alex, for bringing the information because extremely, very deep in terms. I want to thank Astrid for giving us insights into biochemistry. My true patient, Trudy, and my coach over here, Kenna, and the supporting staff. So I want also to go if you guys want to find us. We’re here, and we’re here in this area where we are available. If we can help you and you can contact us at any given time. I want to thank you all, and I appreciate it. We’re going to be hitting sciatica relentlessly because it was relentlessly the scourge. It is ripping apart a lot of people at their works. They just quietly suffer. They don’t sleep, they stress out, and it causes a disruption. And it happens in mommy’s world, and it disrupts the whole family directly because a happy mommy is a happy family. So the entire thing is what we want to do is to assess what’s going on here. Find out the treatment protocols and give you the best options possible. Thank you guys very much, and God bless.
In today’s podcast, Dr. Alex Jimenez and Dr. Mario Ruja discuss what sciatica does to the body and how it affects a person’s overall health and wellness.
What Causes Sciatica?
[00:00:06] Dr. Alex Jimenez DC*: Hey Mario, we’re on a new podcast today. Today we’re going to be talking about sciatica and the complications with that. I got Mario here, and we’ve decided to chat and discuss the issues of sciatica.
[00:00:29] Dr. Mario Ruja DC*: It sounds excruciating.
[00:00:31] Dr. Alex Jimenez DC*: You know, let me ask you this. In your practice, Mario, in terms of working with sciatica, what have you learned over the years in terms of sciatica?
[00:00:41] Dr. Mario Ruja DC*: Sciatica will put you down, Alex. It will make you feel like a baby and make you remember how vital chiropractic is and maintenance. It’s like having that car. For example, if you are driving Buggati and do not do the maintenance, you just put gas. It’s just like, rip it and run it. And then one day, it leaves you hanging in the middle of I-10, and everyone’s passing you, and you’re embarrassed.
[00:01:15] Dr. Alex Jimenez DC*: It is what sciatica is.
[00:01:18] Dr. Mario Ruja DC*: It isn’t very pleasant.
[00:01:20] Dr. Alex Jimenez DC*: You know, I believe it’s kind of funny that we’re laughing at it, but it is a scourge. I call it of the low back. It catches you off a surprise. It creeps up on you. It looms around, too. Yeah. And when they bite you, I mean it classically defined as pain going down the leg. There’s a lot of reasons why that happens. What do you get when your patients show up with that? What do they tell you? What kind of symptoms do they sort of present?
[00:01:45] Dr. Mario Ruja DC*: You got to be kidding me. First of all, their wife drives them in. Does that tell you what it is? Yeah, it’s like a knife stabbing them in the back, and it radiates down their leg, and then they’re usually leaning to one side or another. And then they have this story. Alex, there is this crazy story like, ” Well, I was only…” the only part is ridiculous. “I was only picking up my child,” or “I was only throwing the football, and all of a sudden, my back went out. And then I try to stretch it, and I have my wife rub it. And all of that didn’t work the following day. I couldn’t get out of bed and had to crawl to the bathroom.” Now that is when your attention is on.
[00:02:43] Dr. Alex Jimenez DC*: Yeah.
Dr. Alex Jimenez and Dr. Mario Ruja Explain What Sciatica Does To The Body.
[00:02:44] Dr. Mario Ruja DC*: Our attention is on sciatica. This is a big topic, Alex.
[00:02:48] Dr. Alex Jimenez DC*: This is a vast topic, and let me just kind of throw this out there where we are going to begin the process of breaking down sciatica by no means are we going to be able even to know the breadth and width as this is like saying you can take down a sequoia with one bite. It’s not going to happen, and we’re going to have to chisel away from it. And as we go in there, we’re going to go deep. Are we going to get nasty with the science, Mario?
[00:03:14] Dr. Mario Ruja DC*: This is getting deep and nasty. Folks will have to strap on their seatbelts for this ride.
[00:03:21] Dr. Alex Jimenez DC*: Absolutely. As we do that, we’re going to be able to kind of go deep into it. We’re going to touch on some subject matters, but follow us on this process because we’re going to be discussing real essential issues about sciatica that affects so many millions of people at any given point. I’d venture to say that one in every four people is suffering from chronic back pain, and half of those people are suffering from sciatica in some form or the other or some pain down the leg. So in that sense, we’re dealing with a huge issue that affects millions of patients and millions of people across the country with all different doctors and different types of protocols. And these protocols can be from really esoteric to invasive. And we all want to do it quickly, and we all want to do it a simple way. So I think modern medicine Mario has determined that we have to go basic and try everything before any surgical interventions.
[00:04:16] Dr. Mario Ruja DC*: I mean, it’s common sense, and I always used the car model as an example. Before you get a rebuilt transmission, why don’t you maintain it before you drop a new engine? Why don’t you change the oil and get a tune-up? Unfortunately, again, you mentioned the unbelievable impact of low back pain in our society. I believe I don’t know if I may be in the ballpark. It is the number two or three reasons for work injuries and is one of the biggest reasons for the military to get med boarded out of the military. I mean, this is a big issue that impacts people’s lives, and then you would get into chronic pain management, things like that. But again, if we look at the most critical solution in our life, how can we prevent it? Prevention is the natural utilization of therapeutic arts that decrease the misalignment in the spine. Again, that misalignment is that torque where your back is out of alignment and calibration, right? Which causes uneven wear and tear on the disc. Then the other one is constant compression of sitting down and repetitive motion. The other one is just the injuries from everyday sports activities. More and more young kids are getting injured in sports football, basketball, more intense pain, more torque, and you can see pro basketball players and football players, all of them suffer from sciatica.
[00:06:19] Dr. Alex Jimenez DC*: Yeah. Here’s the cascade. The cascade starts with a decalibration of the pelvis or the hips, or some injury trauma, some space-occupying lesion, or something on this path. I’m going to go ahead and demonstrate here on our pathway, and we’re going to show a little bit of what is in the nerves.
[00:06:43] Dr. Mario Ruja DC*: I love this 3-D model you are showing here.
[00:06:43] Dr. Alex Jimenez DC*: Thank you.
[00:06:44] Dr. Mario Ruja DC*: This is good stuff.
The Sciatic Nerve
[00:06:46] Dr. Alex Jimenez DC*: This is the complete anatomy provided for us and what we can see is a three-dimensional aspect of how and why someone has sciatica. Now when you look at this, Mario, what’s your first take? Because for me, it says it’s a complicated structure when we’re looking at this. When you look at the back, where it comes out, you see this big old cable called the sciatic nerve, but you see so many proximal areas and so many regions that are getting weird.
[00:07:11] Dr. Mario Ruja DC*: That is a lot of moving parts, Alex.
[00:07:15] Dr. Alex Jimenez DC*: Yes, it is. And you know what? One of the crazy things that I’m looking at here is the sacrum.
[00:07:20] Dr. Mario Ruja DC*: And that is the base.
[00:07:21] Dr. Alex Jimenez DC*: That’s the foundation. The way the creator created us was that this is where energy transmits this bone right here. The sacrum, right? But little to the front of it. You have the sacral nerve roots that come out as they form out. You can see on this particular area; you can see the nerve roots coming out as they come in posterior aspect, you can kind of turn this around and we kind of get this little area here and as we rotate this thing, we can see the sciatic nerve as it comes out of what we call the sacral notch. That sacral notches right there is enormous.
[00:08:03] Dr. Mario Ruja DC*: That is crazy.
[00:08:04] Dr. Alex Jimenez DC*: I know, right? So what happens is when you see it here, you can understand that this big ol’ nerve influences the entire creature. You take this thing out, and you have limited the creature’s ability to move. Please look at it as it comes out; you can look from the inferior border to the superior border. You can see why a woman is pregnant; you can determine why this baby could sit in this pelvic cavity here can cause a lot of damage to the sacral nerve.
[00:08:31] Dr. Mario Ruja DC*: Many of them suffer from back pain and sciatica.
[00:08:34] Dr. Alex Jimenez DC*: This is one of the reasons why right here that baby sits and dances in this whole area here. So when we look at this kind of stuff, we can make sense of all the presentations. As you hurt a nerve in one area, you can see that you would hurt as you would do something like this. And the nerve will hurt a distal or pull towards away from it. Once you hurt that region, our goal is to determine the nerve roots going down on that particular area. If this affects all the way down the leg, it will cause pain. Now, you can see in this specific region what goes on.
[00:09:18] Dr. Mario Ruja DC*: This is it now. Now you see that this is what I like, and this is a creation. If you believe in miracles, you stop believing and just realize that you’re one walking. Here’s the sacral sacrum right here, the sacred bone, and that’s why it’s called sacrum because it’s sacred.
[00:09:42] Dr. Alex Jimenez DC*: I didn’t know that. I learned about the scared bone, and it is the base of the spine.
[00:09:48] Dr. Mario Ruja DC*: This is where, as you mentioned, this is where the birth comes out. This is where the next legacy is created. So here is the ilium. OK, so that’s your hip bone. You have two of them. There is symmetry in our bodies, and that’s how God created us in symmetrical synergy. Then right here are pubic surfaces, and then you’ve got the operators right there, and then here is that L5 disc, and this is the one where I would say probably about 80 percent of disc herniations happened right there. So if you want to take a wild guess, this is it right here.
Intervertebral Foramen
[00:10:32] Dr. Alex Jimenez DC*: Let me hone in on that right there so I can bring that in a little bit better.
[00:10:42] Dr. Mario Ruja DC*: This thing is dancing.
[00:10:43] Dr. Alex Jimenez DC*: As Dr. Ruja was explaining, he’s talking about in the disk space of the spine right here.
[00:10:51] Dr. Mario Ruja: Right, so see, that is where you have the IVF.
[00:11:00] Dr. Alex Jimenez DC*: Intervertebral foramen.
[00:11:01] Dr. Mario Ruja DC*: IVF. Interverebral foramen. There it is, and all that is like a fancy word for it. There’s a hole where the right everything comes out.
[00:11:06] Dr. Alex Jimenez DC*: So here we start looking at the hole on the side, and as we look at it right there. You can see where the nerve roots come out right there.
[00:11:29] Dr. Mario Ruja DC*: So at that point, you see it here.
[00:11:35] Dr. Alex Jimenez DC*: Exactly, and as you turn the model.
[00:11:38] Dr. Mario Ruja DC*: OK, right there.
[00:11:41] Dr. Alex Jimenez DC*: That is the nerve right there.
[00:11:43] Dr. Mario Ruja DC*: So this is where how they sit on top of each other right there. Then you can see it from underneath right in there. Now at this point, these nerves, like the fiber optics, are traveling down through these canals and openings and everything. So there are so many places, Alex, that they can be entrapped, compressed, and they can be twisted again. Remember, the big word for us and in our talks is inflammation.
Does Inflammation Causes Problems In The Body?
[00:12:23] Dr. Alex Jimenez DC*: Inflammation yes.
[00:12:26] Dr. Mario Ruja DC*: Deep inflammation, yes. Now, these are all again if you’re looking like an electrician because I love how electricians work. You look at the fiber optics, and you have to trace it and find out where the issue is? Is it up here? Right here? Is it in the middle? Is it here in the canal? It is right there in that notch is the muscle compress.
[00:13:01] Dr. Alex Jimenez DC*: Oh yeah, you can see it in the muscle compress.
[00:13:12] Dr. Mario Ruja DC*: See where it’s pinched right there. That peraforma muscle is now critical. Again, that’s where you see a lot of times you need to release that muscle. Once it compresses, it just goes haywire right there.
[00:13:30] Dr. Alex Jimenez DC*: Yeah, why do they call the peraforma muscle Mario?
[00:13:35] Dr. Mario Ruja DC*: Tell me, Alex.
[00:13:37] Dr. Alex Jimenez DC*: Because it looks like a pear. When you take it, it’s a fat muscle when you look kind of flat here.
[00:13:43] Dr. Mario Ruja DC*: And I visualize in the pear, Alex.
[00:13:44] Dr. Alex Jimenez DC*: Yeah. Here is the top of the pear, and that’s the wide part of the pear.
[00:13:49] Dr. Mario Ruja DC*: That’s cute, Alex. I don’t know what kind of pear that is.
[00:13:52] Dr. Alex Jimenez DC*: Exactly.
[00:13:52] Dr. Mario Ruja DC*: But yeah, you’re right, it’s pear-shaped. Now I can see it.
[00:13:56] Dr. Alex Jimenez DC*: This is a crazy part. There’s a superior Escamilla right here in that area so that it can be trapped anywhere. As we look at this from the base point of view, you can see why people start having these symptoms.
[00:14:08] Dr. Mario Ruja DC*: Yeah, if we look at this pattern, we can also see an increased sedentary lifestyle, Alex. Can you see how all of these muscles are here? The glutes, gluteus minimus, Maximus, the hamstrings. Major squat muscles and the hips. Can you see all of these being deconditioned and compressing on a nerve?
The Lymphatic System
[00:14:40] Dr. Alex Jimenez DC*: Yeah, let me show you this, Mario because I wanted to show you this. When I first started seeing this, I thought this as you begin noticing that you have the venous system, but here’s what people don’t know about the venous system. Next to it is the lymphatic system. Now let me remove these muscles here, and you’re going to see the intricacies of the green lines. These green lines are in the circulatory system.
[00:15:02] Dr. Mario Ruja DC*: Wow, the green lines are the lymphatic system.
[00:15:05] Dr. Alex Jimenez DC*: The green is the lymphatic, and the red is arterial. When you start seeing red now, you can see that they have problems with their circulation when someone sits down a lot. And as you can see here, imagine sitting down all day on top of this thing? Can you see how the inflammation would happen in that region?
[00:15:25] Dr. Mario Ruja DC*: Alex, look at how much is happening in that pelvic area. I mean, this is like fiber optics just strapped, and this is like compress. Already, there is not that much space going on here, Alex. I mean, you’ve got nerves, arteries, veins, and lymph, all of those going through the same canal. So there is not a lot of what I call, you know, space and forgiveness. That’s why this radiating pain down the leg compresses that area that the flow down the leg is activated. That’s why your leg goes numb and your muscles to a large extent after a long time of having this problem. What happens, Alex, with a lot of my patients is they get muscle atrophy. You know, they gain muscle weakness, and that’s where your muscles shrink.
[00:16:40] Dr. Alex Jimenez DC*: Let me show you the additional muscles here. You see, that’s why we train because all these muscles here are surrounding and covering up this area, and the muscle decalibrates.
[00:17:00] Dr. Mario Ruja DC*: Decalibrates.Is that like a fancy word for saying it just…
[00:17:05] Dr. Alex Jimenez DC*: De-conditions?
[00:17:06] Dr. Mario Ruja DC*: That flops down?
[00:17:08] Dr. Alex Jimenez DC*: For me, I like the word calibration because it is a fine-tuned structure. Philosophically speaking, they got a bump at this ball that follows them everywhere when you look at humans. This power unit, right? This throttling system, it’s the glutes. Some have it more significant than others, right? But here’s where we propel from; it is the source of power. It is the way the creature creates its anchor. If the hips are gone, the beast doesn’t survive. So when we look at this, and we look at someone who was an athletic person when they were young and all of a sudden they get this job where they sit in front of a computer, they don’t go out. What happens to them? They decalibrated like a car. It doesn’t get used, and before you know it, it starts sinking and becoming flattered, and eventually, the inner workings that we just came from really start grinding. So when there’s congestion, the lymphatic system is responsible for the circulation. But the lymphatic system, unlike the arterial and venous system, which works primarily with the heart pumping, is functional by motion. So when you sit down, you are not moving.
[00:18:16] Dr. Mario Ruja DC*: You know what, Alex? It is the sacral occipital pump; when you’re talking about the CSF cerebral spinal fluid, I can tell you right now when that sacrum is not pumping back and forth when you’re walking, you know what happens? It’s stagnating to flow to your brain.
[00:18:36] Dr. Alex Jimenez DC*: It does.
[00:18:37] Dr. Mario Ruja DC*: Yeah, all the way to your brain. Then the area that you talked about that I think is critical. You’ve got to keep the body moving. We are created as bipeds. We do not walk like gorillas who walk on all fours. I know sometimes you feel like one, but we’re not apes. That’s right; we’re not silverback apes. The thing is, we’re bipeds. So that means the whole body has to align and stand up. Alex, in every sport, I tell people I’m impressed with your biceps, but your core sucks. You know what? Your core determines your overall function. That is where you keep your body upright, and you create that calibration of your spine. Once that that lordosis, that curve into your back. Once that is lost, you’re degenerating; you’re aging. There it is, right there.
[00:19:41] Dr. Alex Jimenez DC*: Let’s go ahead and take a look at that right there. Yeah, that’s the lordosis you’re talking about in the spine.
The Lordosis
[00:19:56] Dr. Mario Ruja DC*: Can you draw the lordosis out?
[00:19:59] Dr. Alex Jimenez DC*: Of course.
[00:20:01] Dr. Mario Ruja DC*: Wow, that is crazy, Alex.
[00:20:06] Dr. Alex Jimenez DC*: That is crazy.
[00:20:10] Dr. Mario Ruja DC*: OK, so let’s do the pink pen for pain on the lordosis.
[00:20:17] Dr. Alex Jimenez DC*: That curve along with this curve makes a big difference. So what happens is you end up understanding that this sacrum or this glute area influences a vast area. What I’ve learned in my practice is that when you have a person with a sciatic issue, there are upper back issues, and there are shoulder issues now if the lower back has problems…
[00:20:53] Dr. Mario Ruja DC*: It throws everything off, and it’s like a domino effect.
[00:20:56] Dr. Alex Jimenez DC*: Yeah. What do you think about when they tell you, Hey, the person only hurt their lower back, and this is a work-related job? And similarly, they say it’s only related to the back. Yet they come in with leg pain, arm pain, and it makes sense to us, but nobody wants to understand that.
[00:21:11] Dr. Mario Ruja DC*: Yeah, that’s because they don’t want to, Alex. That’s where they want to lie, and it’s a lie. Remember when your mama told you it is not OK to lie?
[00:21:34] Dr. Alex Jimenez DC*: You know what? Why don’t we just say for what it is? They’re lying. They understood why they don’t understand that the body is a biomechanical chain, and if it affects the hips, it starts affecting the lower back, which then affects the upper back. And everybody knows if you have a back that’s giving up, your shoulders will have issues. If you got shoulder problems, it is equally on the opposite side of the room; you’re going to have knee issues. So what happens is as we look at this dynamic model, we see that we can’t be telling a fib here.
The Trapezius
[00:22:06] Dr. Mario Ruja DC*: The spine is one unit composed of many segments. OK, it’s not separate. So there is no way that you can have an injury to one part of the spine, and you can tell me 100 percent that it does not affect any other one. It’s impossible. I’m sorry, God didn’t create it. If you want to see it here, look at this ischium muscle as it goes all the way across. Look at this one. This one is amazing. I’m just going to do this. Here is here’s the muscle right here, trapezius. Now watch as it goes from here to where the shoulders are down, then go to the neck in the back of the neck.
[00:23:32] Dr. Alex Jimenez DC*: Let me clear up the pen marks, OK?
[00:23:35] Dr. Mario Ruja DC*: Can you move the body down?
[00:23:38] Dr. Alex Jimenez DC*: Yes, I can, and there you go.
[00:23:44] Dr. Mario Ruja DC*: So I want to show one example so you can see all the way to the base of the head.
[00:23:49] Dr. Alex Jimenez DC*: OK, I got you.
[00:23:52] Dr. Mario Ruja DC*: Alright.
[00:23:57] Dr. Alex Jimenez DC*: Well, here’s what you want to show. I think what you’re trying to show is that you’re trying to show the negative muscles and see all the good stuff in there.
[00:24:06] Dr. Mario Ruja DC*: Yeah, but I want to show you just that top layer, the trapezius.
[00:24:10] Dr. Alex Jimenez DC*: Oh, let’s go to the muscular portion.
[00:24:11] Dr. Mario Ruja DC*: So it goes all the way from the base. Can you zoom out so we can see the whole thing?
[00:24:16] Dr. Alex Jimenez DC*: Sure can.
[00:24:18] Dr. Mario Ruja DC*: OK, lift the model.
[00:24:20] Dr. Alex Jimenez DC*: I wish I could.
[00:24:23] Dr. Mario Ruja DC*: Now here it is, and this is how dynamic this is. When people say, Oh, you only hurt your neck, but not your mid-back. Here it is. Trapezius right here goes from the base of the skull down the shoulders, right there, all the way down to the mid-back. OK, and this is probably like T10 T11, right? Somewhere around there, right by the middle and all the way across. So this whole area right there, that’s one muscle, and if you have an injury here in this area, this will affect all the way here then if you go in deeper into the second and third layer of the muscle.
[00:25:50] Dr. Alex Jimenez DC*: Let me click here for you to see it.
[00:25:53] Dr. Mario Ruja DC*: Now it gets crazy.
[00:25:55] Dr. Alex Jimenez DC*: When we start removing muscular layers or increasing muscle layers, you start looking at all the functions.
[00:26:02] Dr. Mario Ruja DC*: Oh, look at that, the super spinadeus, And look at this right here. Vader scapula and from the shoulder all the way to the head is scalenus calculus.
[00:26:24] Dr. Alex Jimenez DC*: OK, so what we’re looking at here, we’re looking at the unbelievable body, but let’s go back to the area of concern.
[00:26:33] Dr. Mario Ruja DC*: All right, you see how connected it is, Alex.
What Are The Causes of Sciatica?
[00:26:36] Dr. Alex Jimenez DC*: Here’s the deal, OK? You and I know that the whole darn thing is connected, right? We can determine what is going on after dealing with the many patients we’ve seen over the years. And we’re like violin instructors. We touch the violin, and we make this body move. Our job is to understand when someone comes in and physically to see where this problem is. Find out where the issues are; there are tons of issues, and we haven’t even begun. We’re just having a general conversation about sciatica and where the issues are. What we don’t want is we don’t wish to surgical intervention at any early state unless it’s really necessary. Now what we’re looking at is when we see this, nobody wants that. So how do we fix this? So there are tons of ways to do that.
[00:27:26] Dr. Mario Ruja DC*: Can we go back to the slides of the causation for sciatica?
[00:27:34] Dr. Alex Jimenez DC*: Absolutely. I’m going to take you back to the causation when you get over there in a second. The causation is right here, and we are looking at it.
[00:27:51] Dr. Mario Ruja DC*: The first one is compression.
[00:27:52] Dr. Alex Jimenez DC*: Compression of the disc.
[00:27:54] Dr. Mario Ruja DC*: Compression due to the lack of calibration balance within the system. So you have uneven compression and then a lot of sitting down; we talked about that, right? And then inflammation again, inflammatory process. We spoke last week about metabolic syndrome, inflammation. Inflammation affects the whole body and the disc bulging. Number two right there is disc bulging. That one again is due to what? The spine is out of calibration, out of alignment, putting uneven pressure, and it’s just like squeezing a balloon or a donut. That’s a classic example. You put pressure on a donut on one side, and it will crack, then you go from this bulge to worse herniation. Herniation and then fractures. Of course, if you have trauma DDD, that’s a funny thing. Degenerative disc disease.
Degenerative Disc Disease
[00:28:58] Dr. Alex Jimenez DC*: Yes, early degenerative issues.
[00:29:00] Dr. Mario Ruja DC*: Right? And I love it because most people come into my clinic go, “Oh, I have degenerative disc diseases like I’m getting old,” and I say, “No. You had no maintenance on your back, and you’re not old. ” If you would have taken better care of your body, you wouldn’t have degeneration. They act as though this is normal; however, it is not normal; this is just a sign of the breakdown.
[00:29:23] Dr. Alex Jimenez DC*: You know, the magnitude of either of us uncovering or discovering where a person has an issue. All of these things have ways that we can help it. What’s crazy about it is that we have to go against the grain in our methods because you would not think exercise would be a helpful tool right for this. However, exercise is one of the best things for we have to calibrate that pelvis if it’s appropriate. It’s a herniated disc, and it’s a bad one. We have to go ahead and surgically remove that; if not, we do anti-inflammatories, do we do natural methods, and get that body working and calibrating. Sometimes what happens is these people come in. These individuals are patients who come in and suddenly have a pain that just crept up on them over the last couple of weeks. Sometimes they have a slipped injury, a slipped disc, or even a vertebra that’s been fractured for years and now presents with the issues. Sometimes it’s a neurological presentation. Sometimes it’s a metabolic disorder like metabolic syndrome, and they have an inflammatory condition. What I’ve noticed, and I’m sure you’ve seen it too, is that these people who have sciatica live with this looming monster. It’s almost like a snake that lives in their pants, and when it bites them, it gets their whole leg. It disrupts people’s lives. Figuring out where the cause is is very important. So as we go over these things, I mean, it’s essential to go over the regions. I’ve even seen patients where they come in thinking it was sciatica. And sure enough, it’s sad, but it’s a tumor. And in that situation, we move on too quickly. I got to tell you, in the situations where we’ve had it, we’ve had great teamwork and resolved many issues for a lot of patients.
[00:31:06] Dr. Mario Ruja DC*: That’s the beauty of how we think, Alex. We think in terms of integration. So, just because you have a hammer, everything doesn’t look like a nail. We are chiropractors, but at the same time, we are physicians. And what that means is that we know about physiology, anatomy, neurology, all of that. So we can understand that the pain sensor is not the problem. The pain sciatica is not the problem. We look for the causation of the problem, Alex. And that is in many ways, the misalignment, the compression, the inflammation, the disc bulging again, bone spurs, and many times people will say, Well, I have bone spurs because I’m getting old. No, bone spurs are created because there is a misalignment and lack of calibration in your spine where the body is attempting to self-regulate, self align, and it’s called the wolf’s law. You know, its law is the same principle that deals with the fracture healing fracture where you have pressure, that’s where you have increased calcification. Alex, is that correct?
[00:32:22] Dr. Alex Jimenez DC*: It’s the same thing when you work out; when you work out, you get calluses right because the body responds to stress by increasing and protecting the tissue. The same thing happens with the spine. Suppose it starts unloading improperly, then before you know it, the wolf’s law kicks in, the osteoclast start losing, which are the ones that take away bone, and the osteoblasts start winning. Then you have an increase of bone growth in a direction, usually in the direction of the force. So, in essence, the body tries to protect it, so you can imagine if someone’s going like in the leaning tower. Well, it’s on this side that the body protects it to prevent it from falling over. So, in essence, as we look at these degenerative diseases, we try to get them early on, and we try to mobilize. In most scenarios, we can help the individual by different methods and different techniques. And we use a lot of other methods and techniques to help individuals through this process.
Spinal Stenosis
[00:33:18] Dr. Mario Ruja DC*: I want to go through a couple of points. You know, we’re talking about spinal stenosis. Again, the start of spinal stenosis is the misalignment of your spine, which chiropractic has the beautiful art. This is the art and science of correcting that. So the more alignment, the more clarity, the more balance you have in your spine. The more maintenance you receive to your spine, the less spinal stenosis you will have later on in your life. Or again, spinal stenosis. You know, the other one that we’re looking at is degenerative disc disease or disc herniation. I believe that I look at the body in the 25+ years of my practice; the better maintenance you give your body, the fewer issues, and the less breakdown wear and tear you will have later on in your life. So I look at is that we are anti-aging doctors in terms of biomechanics, so we help the body maintain its optimal function for a more extended period. So that way, when you’re in your 60s and 70s, and 80s, you can walk by yourself without a cane, and you can function. You can do a squat. I love fitness calibration every time, you know. Danny is awesome. With PUSH, Danny is tremendous in terms of a fitness core. And this is where the synergy comes in. The more miles, the more wear and tear, the more pounding you put on your body. The more maintenance you need, the more recovery work. And too many people, Alex, have this idea like, Oh, my back hurts, I just need to squat more. I just need to do more weights. I just need to be in a gym, no. It’s like me telling you I don’t need count maintenance and tune-ups on my car. I just need to drive it more now. So the more miles you put on your bag, the more you squat, the more calibration you need. Why? Because eventually, your body is going to go out of alignment.
[00:35:32] Dr. Alex Jimenez DC*: You know, as we look at disorders, like you said, spinal stenosis. There are many reasons we can have spinal stenosis, from a disc to just arthritic issues. But when we have an individual who suddenly has issues, OK, this is not a sudden, you know, kind of thing that the spinal stenosis doesn’t happen unless it’s a massive disc herniation that occurs in one moment. Yeah, but these things and what we’re talking about spinal stenosis, there are different reasons. And in the treatments are many methods are just, you know, microanatomy. There’s also a laminectomy which is to remove the pressure. But the bottom line is very little wrong with the nerve. The issue is compressive forces. So what do we have to do in the situation where there is a biomechanical imbalance in the pelvic girdle most of the time.
[00:36:20] Dr. Mario Ruja DC*: So it is structure impedes on the nerve.
[00:36:23] Dr. Alex Jimenez DC*: Yes. And as we do that, we evaluate that there are certain things like age, obesity, or even less of a life of activity. What are other things, Mario?
What Are The Occupations That Cause Sciatica?
[00:36:33] Dr. Mario Ruja DC*: Sedentary lifestyle, repetitive occupational motion?
[00:36:36] Dr. Alex Jimenez DC*: What kind of occupations would have sciatica?
[00:36:40] Dr. Mario Ruja DC*: Truck drivers. Why? By sedentary vibration. Eight to ten hours by sitting down. Secretaries, I mean, you can go on and on, people working in banks and teachers even.
[00:36:57] Dr. Alex Jimenez DC*: We have patients that go to the Southern Union railroad, the engineers, the vibration, the bouncing over 30 years of vibrating. Eventually, the bone activates the spine clouds, or you have spinal stenosis, and they have back disc issues, and they have degenerative diseases.
[00:37:14] Dr. Mario Ruja DC*: Athletes have a repetitive toque like a golfer. How many golfers do you know that have no back pain? None. How about baseball players?
[00:37:25] Dr. Alex Jimenez DC*: How about our buddy, Tiger Woods?
[00:37:27] Dr. Mario Ruja DC*: Yeah, what happened to him?
[00:37:28] Dr. Alex Jimenez DC*: Yeah, what did people think? People thought he might have been having some issues with alcohol. Still, the reality is he’s taking medication after surgery, and suddenly, he’s driving, and he probably forgot to take medicine. You know, they took a pill and started to get addicted, and this is the issue. We got to figure out how to fix these issues calibrating. But I got to tell you; there are a lot of ways we can help people. The issue is that once we understand where the problem comes from, the plan of attack can take off. There are different issues and different types of diagnoses. We have here a little bit of a window where you can take a look at that. You can see that sciatica is a symptom. It’s a presentation of syndromes. It’s a pain down the leg, but there are tons of reasons.
[00:38:14] Dr. Mario Ruja DC*: Now the causation is right there, right?
[00:38:17] Dr. Alex Jimenez DC*: Well, look at all of these things, and it is ridiculous.
[00:38:21] Dr. Mario Ruja DC*: Wow.
[00:38:22] Dr. Alex Jimenez DC*: The one people think about a lot is peraforma syndrome, and that’s only one component. Then when that doesn’t work, your little stretches, you try to figure out what’s causing it could be tendinopathy, it could be bursitis. Look at all these issues when we go in here; when we look at these particular issues, we can look at other subsequent areas causing problems. You mentioned it before the four sets; this degeneration redevelops the quadrant is formoral area.
[00:38:48] Dr. Mario Ruja DC*: So let’s make this simple. Otherwise, you know, people will listen to us and go; it’s a lot. It’s a lot, and this is like a fire hydrant, and I just have my mouth over it. Alex, this is what we got. Number one, it all comes down to foundation and function, right? If we go back on each of these things from, you know, four-set syndrome, this degeneration, ridiculous hip, you know, formoral impingement, quadrennial femoral, you know, abnormalities all of these. The root of all of these is the misalignment and lack of calibration of the neuromuscular system. I mean, when you go down to it, the majority, I’m not saying 100 percent, let’s not do that. Let’s not be silly tonight. No. The point is the majority, if we can do a better job for our community, if we can do a better job in terms of our athletes, is to create a maintenance calibration system for them, we would decrease a lot of these degenerative disc diseases and diagnoses, we would stop them before they blow up in their face.
Different Methods To Treat Sciatica
[00:40:19] Dr. Alex Jimenez DC*: Let me ask you this. What kind of things in terms of our diagnostic abilities, what we use different methods to diagnose?
[00:40:26] Dr. Mario Ruja DC*: I love MRI.
[00:40:28] Dr. Alex Jimenez DC*: In terms of sciatica, X-rays are good, but MRIs can tell you what the problem is.
[00:40:34] Dr. Mario Ruja DC*: That’s it, and we’re talking about like a Tesla ten. I don’t know if they have it, and I think it’s sorry about it. I just got crazy tonight. Nah, they didn’t make it. We’re going to get some calls. Tesla, what?
[00:40:46] Dr. Alex Jimenez DC*: We got a great radiologist, and they help us hone in on particular areas.
[00:40:54] Dr. Mario Ruja DC*: They have a three-point-o or something?
A Relationship With Your Radiologist
[00:40:59] Dr. Alex Jimenez DC*: The whole idea is a relationship with our radiologists. Our radiologists are our eyes and ears on the deep tissues. I can tell you that we do have the best radiologists working with us. We do. I mean, the city has some top-end radiologists people, and when we send them to them, they communicate with us and tell us where the problem is that from there we go at it from once we know where it’s at. We use cat scans. We use ultrasound. We use bone scans.
[00:41:29] Dr. Mario Ruja DC*: Why is it a question? OK, this is going to get a little crazy and a little nasty tonight. Why is it that most doctors, Alex order X-rays first? Why is it? I can never understand for myself. You know what I tried to go straight to the issue was to go to MRI. Why is it?
[00:41:51] Dr. Alex Jimenez DC*: The standard of care is many insurance carriers will want an X-ray first to see if it’s a degenerative bone structure to be able to bleed on that. But we all understand that the best possible option for actually assessing it is to kind of rule out some things. If you want to look at bone, you do a cat scan to do the soft tissues. Well, this is soft tissue. So then you do an MRI with contrast, and you can see the deep tissues and the separation and the inflammation for any prolonged issues occurring.
[00:42:21] Dr. Mario Ruja DC*: That’s why, to me, Alex, that makes sense if we’re looking at diagnosing disk and nerve issues, right? Why is it that we use an instrument many times and I see this and agree with you. All of the insurances are going in and saying, Hey, you need to do an X-ray first. We won’t let you do the MRI, do they? I’m like, but X-rays don’t show any soft tissues.
[00:42:46] Dr. Alex Jimenez DC*: I think it’s a common thing. It’s almost like when you go to a dentist, you know, they scan all the teeth. It’s pretty easy to generalize. You know, there are times when the standard of care is into that today? For the low back, the standard of care is an X-ray as an initial entry point. So from there, I’ve learned, and I have gotten this lately, that most insurance carriers are very open to allowing the individual based on a presentation to do whatever it takes. They don’t stop. That’s a real beautiful change that’s happened since I’d say for the last five years; it’s a whole different game. So we get to see that we do nerve conduction and nerve testing to see the speed at which the nerve pulses. So we can find that AMG’s electromyography and see how the muscles are. But you don’t need to be doing that stuff for sciatica when you know the person is in severe pain. Now, if you want to prove it, that’s when you do the NCBI. Other than that, the person will not come in telling you that they have pain. Now sciatica because I call it the scourge because it just annoys you. It stops you from doing, you don’t sleep, you get to lay down, and the darn thing just activates. And there you got this electric current preventing you sleep. People come in with their eyes bloodshot and unable to enjoy their lives. This changes the quality, and we need to fix these things.
Does Sciatica Cause Inflammation?
[00:44:09] Dr. Mario Ruja DC*: It affects families. Alex, let’s get down to it. You know what? It affects your relationship with your spouse, with your children, at work. You know, you go to work, and you’re angry. Yes, you’re just mad at the world, and people are trying to figure out, like, what’s wrong, man? And it’s like, “You know what? I’m dealing with stuff.” And then that chronicity after a while, you’re like, “I don’t know what to do. I’m taking too many meds. I’m taking 800 milligrams every day for like five months.”
[00:44:39] Dr. Alex Jimenez DC*: Let’s give the people out there who may want some information a little bit of insight into the other options they have. Because what’s the name of the game here? What are sciatica and inflammation? It’s what it always has and always will be. So what we got to do is do what we can, and many people ask me, What are my options? Well, we have here a breakdown of certain things, and we’re going to discuss these things in real extensive detail over the next couple of months. And we’re going to hit this thing as we will be dealing with sciatica and vitamin C, D, calcium. We’re going deep all these things, you can take a screenshot of this, and you can say berberine. We got glucosamine, ACL, carnitine, alpha-lipoic acid, ashwagandha, soluble fiber, vitamin E, green tea, turmeric. A lot of these things have a lot to do with metabolic syndrome. But guess what? When you have metabolic syndrome, which is what?
[00:45:36] Dr. Mario Ruja DC*: Inflammation.
[00:45:37] Dr. Alex Jimenez DC*: So what we’ve noticed, Mario, and correct me if you see something different.
Ashwagandha
[00:45:44] Dr. Mario Ruja DC*: I love that word ashwagandha.
[00:45:47] Dr. Alex Jimenez DC*: Yeah, I love it too.
[00:45:55] Dr. Mario Ruja DC*: It’s like, we’re going to meditate pretty soon, Alex.
[00:46:01] Dr. Alex Jimenez DC*: So, as we kind of look at these options, we really can discuss deep levels of biomedical science here, OK. Because everyone wants to know what we can do, but since we’re dealing with, let’s say, just on the angle of metabolic syndrome, again, we got to tie in another beast insulin. Insulin inflammation susceptibility. And here, we correlate. It may seem far away, but if you take a hundred people with metabolic syndrome, these people are susceptible to sciatica and the stuff we hold on to.
[00:46:46] Dr. Mario Ruja DC*: Let’s make it simple. How many people do you know with metabolic syndrome that don’t have back pain or sciatica? OK, let’s make it. Let’s make it simple.
[00:46:58] Dr. Alex Jimenez DC*: We got to tie together, and this is where we do it. National in clinical practice, what we do is we make these connections. And the bottom line is we start changing people’s habits, you know, simple things like instead of having a pop or something else only option you should have as green tea. Green tea is an antioxidant anti-inflammatory. We start changing the metabolic processes, begin cutting the gut grease, and all that starts happening.
[00:47:27] Dr. Mario Ruja DC*: OK. We’re mixing ashwagandha with gut grease. You know what? People are going to remember this forever, Alex.
[00:47:34] Dr. Alex Jimenez DC*: If you kind of see what we’re got, we’re saying it is complex. We can go down one rabbit hole and say we got the moment of truth or the thing that’s important. But the reality is that the low back causes neck pain. A lot of people will look at it and say, Why does that happen? Well, as Mario said, you know, God didn’t name it as neck pain. God didn’t call it lumbar spine. We named it the vertebral column. It’s the whole darn thing that is connected. From the moment you heal, strike your head feels the shockwave, right? So when we look at that, when we assess that, we can see that the body has a massive implication when some large nerve, late-deciding nerve, gets offset. So what we can do is first figure out, mitigate the issues, control them and come up with a treatment plan that works appropriately for the patients. So as we do these things, we will go over all those beautiful ideas that we have going on here. And I just wanted to let you know that we’re going to be discussing many more subject matters.
Vitamin D3
[00:48:35] Dr. Mario Ruja DC*: There it is vitamin D3. That is why I love vitamin D3, and it’s everywhere.
[00:48:43] Dr. Alex Jimenez DC*: Four hundred disorders. A 400 percent decrease in all risk mortality or times decreases disease mortality with vitamin D. This is like the magical thing? I mean, common sense. I mean, what’s our biggest organ, right? It’s the skin. So when we live in the sun city, right, what happens?
[00:49:07] Dr. Mario Ruja DC*: We absorb the sun’s rays.
[00:49:09] Dr. Alex Jimenez DC*: And that should be the healthiest.
[00:49:11] Dr. Mario Ruja DC*: Hey, I want to get crazy tonight. All right. Sun City vitamin D. We should be the healthiest on the planet.
[00:49:22] Dr. Alex Jimenez DC*: That’s it. I mean, it’s essential. So what did we get called about a couple of decades ago? Mario, you remember that we were named the fattest sweaty town in the country?
[00:49:35] Dr. Mario Ruja DC*: That angers me, and that should motivate and pump people up. That right there should be the wake-up call and the battle cry of El Paso and the whole region. Never again will you ever open your mouth and say that because we are the best.
Treatment Protocols
[00:50:00] Dr. Alex Jimenez DC*: We are. We are very family-based and a location and a community, but we suffer from metabolic syndrome, which implicates issues. And one of them is sciatica. I got to tell you; there isn’t a day that half my patients coming in have sciatica, and you and I have been doing this between 25 and 30 years, right? So as we’ve been pounding and fixing these disorders. And you’ve got to tell you there are studies where we see that when doctors of all different sorts refer for a surgical consult, there’s a high tendency to have surgical, you know, focus when you go to a nonmusculoskeletal special like a physical therapist or chiropractor, we kind of filter out the situation when in our path or an available position to see the lower back pain. They throw it into the orthopedic surgeon, and only five to 10 percent of most studies show that those become surgical the ones we send. About 50 percent are surgical. That means we do a great job of filtering out before they have that issue. In other words, we fix the problem, and the ones we do refer to these.
[00:51:17] Dr. Mario Ruja DC*: Yes, that’s right.
[00:51:19] Dr. Alex Jimenez DC*: Game on. So we want to make sure you know that you know that we need that for your orthopedist out there. We require that option, that modality, but we don’t do that kind of procedure. But it’s necessary for terms of the common treatment protocol, you know, the mainstay of sciatica.
[00:51:38] Dr. Mario Ruja DC*: It’s gabapentin. Just adding on to that, we refer to real cases, you know? When someone comes in, they need it. It’s not like, Oh, you know what? We’re going to waste people’s time. They need it. Because again, the new model now for back problems and especially sciatica is noninvasive. OK, noninvasive care first for at least two to three months.
[00:52:10] Dr. Alex Jimenez DC*: Well, you know, I’m on my point of view on those guidelines. You know, every person is different.
[00:52:17] Dr. Mario Ruja DC*: Yeah. ODG guidelines, Alex.
[00:52:21] Dr. Alex Jimenez DC*: And what happens is that you can oversee the treatment protocols when we look at these dynamics.
[00:52:31] Dr. Mario Ruja DC*: Yeah, there it is. The treatment protocols. You know, I look at treatment. Chiropractic care, a lifestyle change. Metabolic syndrome, we’re looking at physical therapy; we need everyone on board. Acupuncture, drugs again. Medication for pain. Anti-inflammatory muscle relaxers. Nutraceuticals, herbals, steroid injections. Yeah, those are what we call lying like the second you, even with a lot of the patients, it’s after conservative care by the time they get to that phase. And then, of course, you have surgery, surgical procedures. So yeah, you must go with our patients. We go from noninvasive to invasive care.
[00:53:36] Dr. Alex Jimenez DC*: These procedures are the ones we do.
[00:53:47] Dr. Mario Ruja DC*: Now with those. And that’s a foam roller right at the storm rolling, that means releasing the goods, the pure performance right there. And again, a lot of our viewers will think, hold on. I can’t even walk, and I can’t do that. But again, this is the secondary phase, Alex. This is the second phase. Furthermore, we’re not getting people out, and all of a sudden, they can’t walk in there. They’re, you know, doing box jumps. No, this is the secondary self first care correct release the pressure brake and the pain pattern and then stabilize and correct the muscle imbalance. So those are things because I think a lot of times, you know, many people ask me like, “Oh, you know what? I want to go work out.” I’m going on like, Hey, slow down, superstar, let’s not workout. You know, let’s not work out. Let’s correct the problem. Calibrate your back. Then you work out, and then you do a process of what I call periodicity. That means you scale it. You got to crawl before you walk and walk before you run. So let’s not be superheroes, and a lot of people just aren’t patient.
[00:55:08] Dr. Alex Jimenez DC*: I agree with you.
[00:55:09] Dr. Mario Ruja DC*: They’re not patient. They want things now. You know this has been created. This sciatica and back problems have been created for years. No maintenance for like 10 20 years. And they expect to walk into the office and, in one visit, do jumping jacks. You know what? Sorry but it’s not going to happen. So that’s where people want again. We do our best, but we don’t look for quick fixes. If you wish for the symptoms to go away but are not corrected, then you’re going to deal with the problem. That’s going to be lingering for years and years, and it’s going to get worse, you know, and those pain sensors. This is what’s so important. God created a body such as such a miraculous system, and we can’t even duplicate this. The most potent technology developed to wear the sensors, the awareness, proprioception within our body, and pain is effective. I often tell people, don’t block the pain because it is healthy because it tells you to stop. That pain is that red light on your dash that says, don’t drive the car, don’t park it, and fix it. Please don’t unplug the light and keep driving it. And this is where our society and our, you know, immediate care. I want things now. I can’t wait. Just like fitness, you know, people want to get fit in like like a week.
[00:56:47] Dr. Alex Jimenez DC*: Like, come on, it’s not going to happen.
Conclusion
[00:56:50] Dr. Mario Ruja DC*: Same thing with your health. It takes time, and you have to get the proper diagnosis. You know, the intense lab work, the genomics, the inflammatory. I mean, this is like I tell people, you’ve got to invest in your health or your sickness. Either way, you’re going to spend the money, either way, but once, you’re going to enjoy the fruits of that investment. The other one, you’re just going to drag. So the process of diagnostics from MRI’s, the process of diagnostics to look at metabolic syndrome, to look at your inflammatory process, that’s an investment. And then with those tools with that information, you got to have created baselines, Alex. If you don’t know where you’re at, you don’t know where you’re going. Now that’s what I would say is I want to motivate and empower people to invest in that process because it’s not an overnight thing and people want it. I tell them that they have got to understand. Be disciplined, be relentless and see the results for life instead of patching up your health.
[00:58:15] Dr.Alex Jimenez DC*: This is very dear and near to all of us here because sciatica affects so many individuals. We’re going to be discussing all these issues one section at a time. We’re going to bring an explanation. We’re going to give you an answer. We’re going to provide you with options. We’re going to provide you with treatments. We’re going to come up with a way that we’re going to find the best possible treatment protocol for you. And if not, we’re going to give you at least a basis to ask your doctors exactly what the best approach is, and you’re going to at least know the different directions you can take because we must understand this disorder. It may be simple to many people, but it debilitates you. You integrate way when you have it. We’re going to bring this to you. If you ever want to ask us personal questions and call us personally, Mario makes himself available 24-7 via phone number (915)494-4468. Always has been, and you get called all the time as he is right now. My phone number is(915)850-0900. And here we have, Mario, and I want to thank you all for allowing us to go over these things. This is also Mario’s website at: rujahealth.com. It’s easy, and it’s a fantastic site. We got me over here. This is my address and my phone, and then there’s Daniel Alvarado, where he works from the PUSH Fitness center. So we welcome you guys to see what’s cooking here and seeing what’s happening, and we wish you the best of everything that’s happening. So as we go through that. Mario, it’s been a blessing, brother and I look forward to going over more details with you in the next couple of days, and we will start recording more and more as time goes on. God bless.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine