
Can exercise slow down the progression of multiple sclerosis? Multiple sclerosis, or MS, is a chronic, neurological disease characterized by damage to the myelin sheaths of nerve cells in the central nervous system, or CNS. Common symptoms of multiple sclerosis include pain, fatigue, vision loss and impaired coordination. Exercise is frequently recommended as a form of treatment for several types of injuries and/or conditions, including MS. While exercise has been determined to help improve the management of symptoms of multiple sclerosis as well as decrease the progression of the disease, further evidence is still required. The purpose of the following article is to demonstrate how exercise can affect disease progression of multiple sclerosis and improve quality of life in patients.
Contents
Abstract
It has been suggested that exercise (or physical activity) might have the potential to have an impact on multiple sclerosis (MS) pathology and thereby slow down the disease process in MS patients. The objective of this literature review was to identify the literature linking physical exercise (or activity) and MS disease progression. A systematic literature search was conducted in the following databases: PubMed, SweMed+, Embase, Cochrane Library, PEDro, SPORTDiscus and ISI Web of Science. Different methodological approaches to the problem have been applied including (1) longitudinal exercise studies evaluating the effects on clinical outcome measures, (2) cross-sectional studies evaluating the relationship between fitness status and MRI findings, (3) cross-sectional and longitudinal studies evaluating the relationship between exercise/physical activity and disability/relapse rate and, finally, (4) longitudinal exercise studies applying the experimental autoimmune encephalomyelitis (EAE) animal model of MS. Data from intervention studies evaluating disease progression by clinical measures (1) do not support a disease-modifying effect of exercise; however, MRI data (2), patient-reported data (3) and data from the EAE model (4) indicate a possible disease-modifying effect of exercise, but the strength of the evidence limits definite conclusions. It was concluded that some evidence supports the possibility of a disease-modifying potential of exercise (or physical activity) in MS patients, but future studies using better methodologies are needed to confirm this.
Keywords: disease activity, exercise therapy, physical activity, training
Introduction
Multiple sclerosis (MS) is a clinically and pathologically complex and heterogeneous disease of unknown etiology [Kantarci, 2008]. In 28 European countries with a total population of 466 million people, it is estimated that 380,000 individuals are affected with MS [Sobocki et al. 2007]. The disorder is progressive but more than 80% of all MS patients have the disease for more than 35 years [Koch-Henriksen et al. 1998], the number of years of life lost to the disease being 5 to 10 [Ragonese et al. 2008]. The fact that MS is a chronic, long-lasting and disabling disease makes MS rehabilitation an important discipline in maintaining an independent lifestyle and the associated level of quality of life [Takemasa, 1998]. Despite the fact that MS patients for many years were advised not to participate in physical exercise because it was reported to lead to worsening of symptoms or fatigue, it has become generally accepted to recommend physical exercise for MS patients during the last two decades [Sutherland and Andersen, 2001]. Exercise is well tolerated and induces relevant improvements in both physical and mental functioning of persons with MS [Dalgas et al. 2008]. It is an open question whether exercise can reverse impairments caused by the disease per se, or whether exercise simply reverses the effects caused by inactivity secondary to the disease. However, most likely exercise may reverse the effects of an inactive lifestyle adopted by many patients [Garner and Widrick, 2003; Kent-Braun et al. 1997; Ng and Kent-Braun, 1997; Stuifbergen, 1997]. Nonetheless, it has been suggested that exercise might have the potential to have an impact on MS disease progression by slowing down the disease process itself [Heesen et al. 2006; Le-Page et al. 1994; White and Castellano, 2008b]. In other disorders exercise has been shown to pose the potential to have an impact on brain function and, as recently summarized by Motl and colleagues, exercise in older adults with or without dementia leads to cognitive improvement relative to a control condition [Motl et al. 2011b]. Based on this and the few existing findings in MS patients, Motl and colleagues suggested that exercise may similarly improve cognitive functioning in MS patients. However, in MS it has not been reviewed whether physical exercise has a more general disease-modifying effect.
To gain more insight on this important topic, we therefore conducted a systematic literature search aiming at identifying studies linking exercise (or physical activity) to disease progression in MS patients or in the experimental autoimmune encephalomyelitis (EAE) animal model of MS. A secondary purpose of the review was to discuss possible mechanisms explaining this link if it does exist and to discuss future study directions within this field.
Methods
The included literature was identified through a comprehensive literature search (PubMed, SweMed+, Embase, Cochrane Library, PEDro, SPORTDiscus and ISI Web of Science) that was performed in order to identify relevant articles regarding MS and exercise up to 4 September 2011. The search was performed using the subject headings �exercise�, �exercise therapy�, �physical education and training�, �physical fitness�, �motor activity� or �training� in combination with �multiple sclerosis� or �experimental autoimmune encephalomyelitis�. No limitations regarding publication year and age of subjects were entered. If possible, abstracts, comments and book chapters were excluded when performing the search in the different databases. This search yielded 547 publications. A screening of these publications based on title and abstract revealed 133 publications relevant for further reading. The reference lists of these 133 publications were checked for further relevant publications that were not captured by the search. This resulted in further six publications and in a total of 139 closely read publications. Studies that turned out to be nonrelevant (n = 65), meta-analyses (n = 3), reviews (n = 22), conference abstracts (n = 8) and articles not written in English (n = 2) were excluded from the final analysis (see Figure 1). Relevant cross- sectional and longitudinal studies were included.
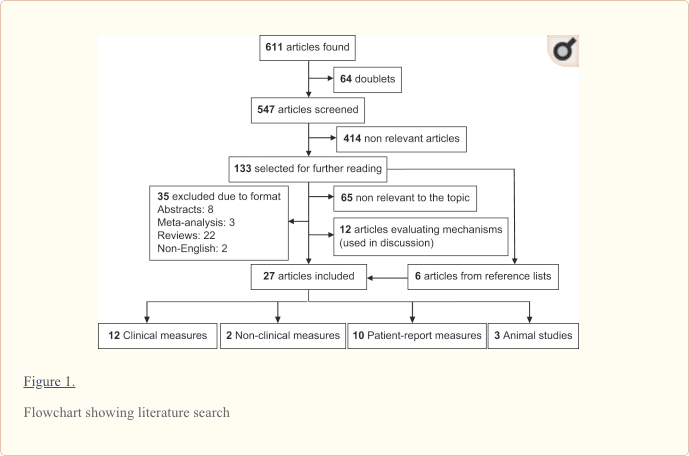
According to Goldman and colleagues measures thought to reflect disease progression (or activity) in MS can be evaluated with objective or subjective outcome measures [Goldman et al. 2010]. Objective measures include (1) clinical outcome measures such as the Expanded Disability Status Scale (EDSS) and Multiple Sclerosis Functional Composite (MSFC) and (2) nonclinical measures such as MRI. The subjective measures include (3) patient-reported measures thought to reflect disease progression or disability such as the Late-Life Function and Disability Inventory. Studies applying patient-reported measures that included a measure of physical activity were also included in this category. Furthermore, we added a category containing studies applying (4) the EAE animal model of MS as study population. Based on this framework the localized articles were divided into the following four groups (see Table 1):
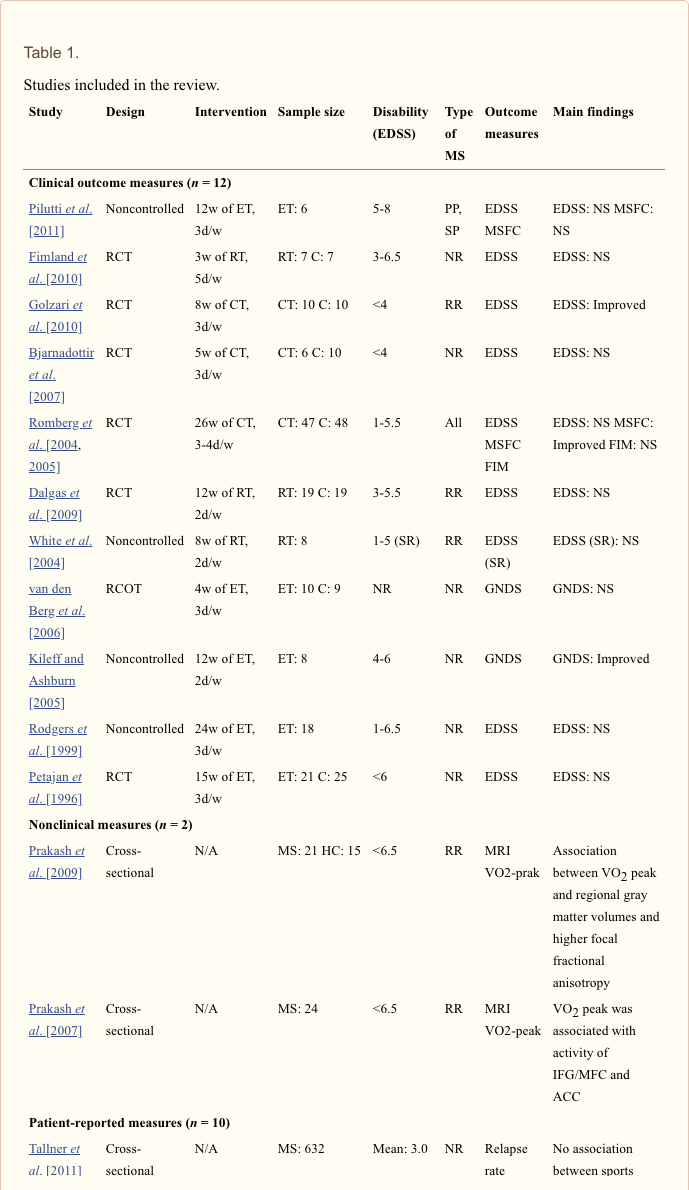
- disease progression evaluated with clinical outcome measures (n = 12);
- disease progression evaluated with nonclinical measures (n = 2);
- disease progression evaluated with patient-reported measures (n = 10);
- disease progression evaluated in animal studies (n = 3).
Results
Disease Progression Evaluated with Clinical Measures
A number of studies evaluating structured exercise interventions lasting from 3 to 26 weeks have included clinical scales reflecting disease progression as an outcome measure. The applied clinical scales include the EDSS [Bjarnadottir et al. 2007; Dalgas et al. 2009; Fimland et al. 2010; Golzari et al. 2010; Petajan et al. 1996; Pilutti et al. 2011; Rodgers et al. 1999; Romberg et al. 2004; White et al. 2004], the MSFC [Pilutti et al. 2011; Romberg et al. 2005], the Guys Neurological Disability Scale (GNDS) [Kileff and Ashburn, 2005; van den Berg et al. 2006] and the Functional Independence Measure (FIM) [Romberg et al. 2005]. Studies applying the EDSS have generally not found any change after either endurance training [Petajan et al. 1996; Pilutti et al. 2011; Rodgers et al. 1999], resistance training [Dalgas et al. 2009; Fimland et al. 2010; White et al. 2004] or combined training interventions [Bjarnadottir et al. 2007; Romberg et al. 2004]. Only one study by Golzari and colleagues evaluating the effects of 8 weeks of combined training (3 days/week) reported an improvement in EDSS score [Golzari et al. 2010]. This finding was not confirmed in a long-term study (26 weeks) [Romberg et al. 2005] also evaluating the effects of combined training. In the study by Romberg and colleagues no effect on EDSS and FIM were found, but a small positive effect was seen in the MSFC. A few studies applied the GNDS with one reporting an improvement after 12 weeks of biweekly endurance training [Kileff and Ashburn, 2005] and one reporting no effects of 4 weeks endurance training completed 3 days a week [van den Berg et al. 2006].
In summary, structured exercise intervention studies of different exercise modalities lasting 3�26 weeks have generally found no effects on EDSS scores. A few exercise studies have shown positive effects when applying other clinical scales (MSFC and GNDS).
Disease Progression Evaluated with Non-Clinical Measures
Two studies by Prakash and colleagues have evaluated the effects of cardiorespiratory fitness on brain function and structure by applying (functional) MRI [Prakash et al. 2007, 2009]. One study [Prakash et al. 2007] investigated the impact of cardiorespiratory fitness on cerebrovascular functioning of MS patients. Twenty-four female participants with relapsing�remitting MS were recruited for the study and all participants went through fitness assessment (VO2 peak) and were scanned in a 3-T MRI system while performing the Paced Visual Serial Addition Test (PVSAT). Higher fitness levels were associated with faster performance during the PVSAT that could be related to greater recruitment of a specific region of the cerebral cortex (right inferior frontal gyrus [IFG] and middle frontal gyrus [MFG]) known to be recruited by MS patients during performance of PVSAT to purportedly compensate for the cognitive deterioration attributable to MS. In contrast, lower levels of fitness were associated with enhanced activity in the anterior cingulate cortex (ACC), thought to reflect the presence of a larger amount of conflict increasing the potential for error in lower fit MS participants. The authors interpreted the results as supporting aerobic training as an intervention to support the development of additional cortical resources in an attempt to counter the cognitive decline resulting from MS. Among a number of cognitive tests, only the Paced Auditory Serial Addition Test (PASAT) showed a weak correlation (p = 0.42) to VO2 peak leading the authors to suggest that fitness does not have an influence on measures of general cognitive functioning.
In another study by Prakash and colleagues the relationship between cardiorespiratory fitness (VO2 max) and measures of gray matter atrophy and white matter integrity (both of which have been associated with the disease process) were studied [Prakash et al. 2009]. A voxel-based approach to analysis of gray matter and white matter was applied on brainscans from a 3-T MRI system. More specifically it was examined whether higher levels of fitness in 21 female MS patients were associated with preserved gray matter volume and integrity of white matter. A positive association between cardiorespiratory fitness and regional gray matter volumes and higher focal fractional anisotropy values were reported. Both preserved gray matter volume and white matter tract integrity were associated with better performance on measures of processing speed. Recognizing the cross-sectional nature of the data, the authors suggested that fitness exerts a prophylactic influence on the structural decline observed early on, preserving neuronal integrity in MS, thereby reducing long-term disability.
In summary, (f)MRI studies suggesting a protective effect of cardiorespiratory fitness on brain function and structure in MS patients have started to emerge. However, the cross-sectional nature of the few existing studies limit conclusions regarding the existence of a causal relationship.
Disease Progression Evaluated with Patient-Reported Measures
A number of studies have addressed the relationship between exercise or physical activity and disease progression in large-scale questionnaire studies applying patient-reported measures.
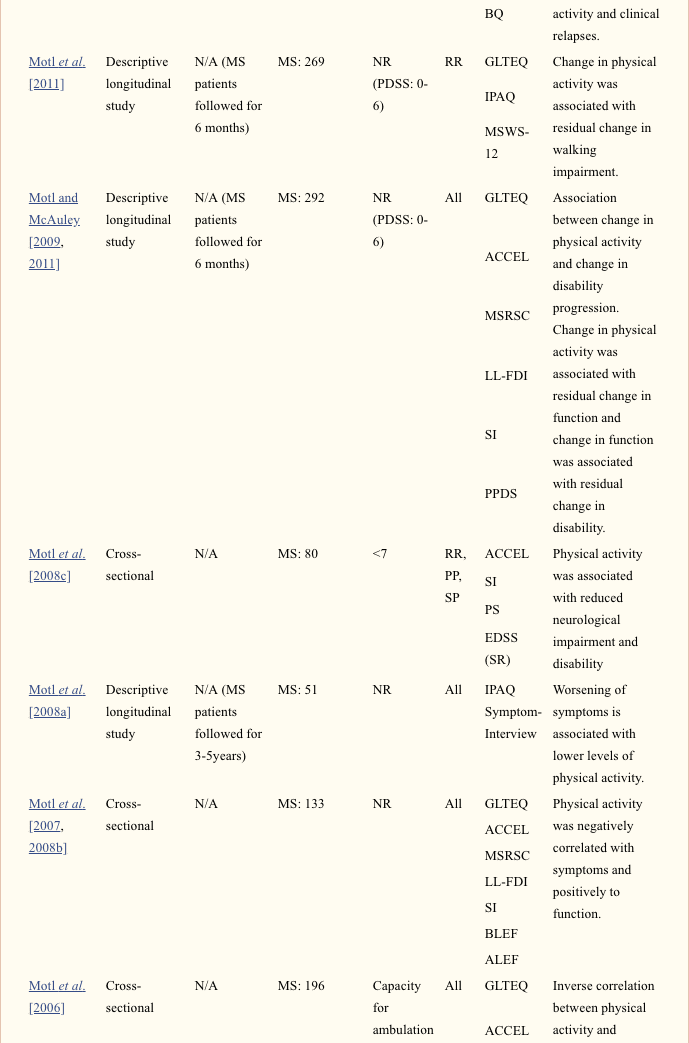
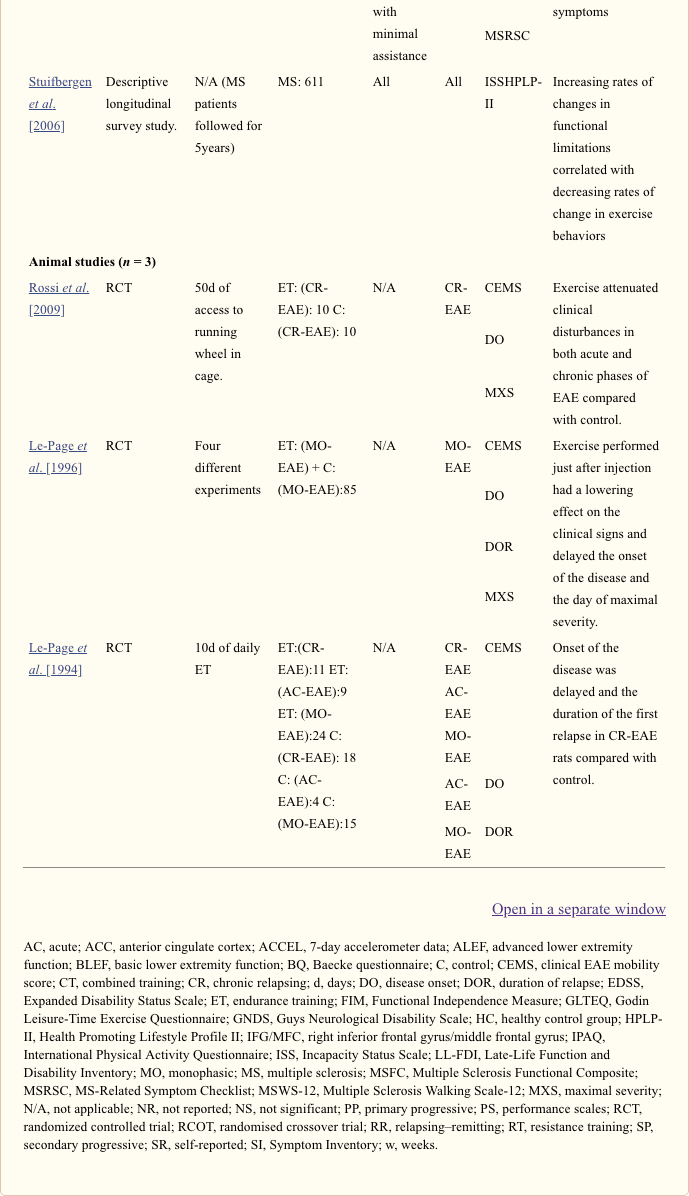
In a large descriptive longitudinal survey study, Stuifbergen and colleagues examined the correlations between the change in functional limitations, exercise behaviors and quality of life [Stuifbergen et al. 2006]. More than 600 MS patients completed a number of questionnaires every year for a period of 5 years. The self-reported longitudinal measures were analyzed by applying latent curve modeling. The Incapacity Status Scale provided a measure of functional limitations due to MS, whereas the Health Promoting Lifestyle Profile II provided a measure of exercise behavior. At the first test point (baseline test) cross-sectional data showed a significant negative correlation (r = ?0.34) between functional limitations and exercise behaviors, suggesting that at the start of the study higher levels of functional limitations were associated with lower levels of exercise. Longitudinal data from the study showed that increasing rates of changes in functional limitations correlated with decreasing rates of change in exercise behaviors (r = ?0.25). In other words these findings are suggesting that increases in exercise behaviors correspond with decreased rates of change in functional limitations. No correlation between the initial degree of limitation and continuing rate of exercise was found which led the authors to suggest that persons with MS with varied levels of limitations might slow the trajectory of increasing limitations over the long term with consistent exercise participation.
A series of studies from Motl and colleagues have addressed the relationship between physical activity, symptoms, functional limitations and disability in MS patients. In a cross-sectional study [Motl et al. 2006] in 196 MS patients, the number of symptoms within 30 days (MS-related Symptom Checklist) and physical activity (Godin Leisure-Time Exercise Questionnaire and 7-day accelerometer data) were collected. After modeling data a direct relationship between symptoms and physical activity were found (r = ?0.24) indicating that a greater number of symptoms resulted in lower amounts of physical activity. However, the authors noted that the cross-sectional design precludes inferences about the direction of causality, and physical activity might affect symptoms as symptoms affect physical activity participation. When modeled this way a moderate inverse correlation between physical activity and symptoms was found (r = ?0.42) indicating fewer symptoms when the physical activity level is high. This led the authors to suggest the existence of a bi-directional relationship between physical activity and symptoms.
In a following questionnaire study Motl and colleagues examined physical activity (Godin Leisure-Time Exercise Questionnaire and 7 day accelerometer data) and symptoms (Symptom Inventory and MS-related Symptom Checklist) as correlates of functional limitations and disability (Late-Life Function and Disability Inventory) in 133 MS patients [Motl et al. 2007, 2008b]. A model based on the disablement model proposed by Nagi (1976) was tested as the primary model and this showed that physical activity and symptoms were negatively correlated (r = ?0.59) and those who were more physically active had better function (r = 0.4). Furthermore, those with better function had less disability (r = 0.63) which led the authors to conclude that the findings indicate that physical activity is associated with reduced disability (through an association with function) consistent with Nagi�s disablement model (Nagi 1976), but again the cross-sectional design limited definite conclusions on the direction of the relationships.
Motl and colleagues then published a longitudinal (case report) study examining the relationship between worsening of symptoms and the level of physical activity throughout a 3- to 5-year period [Motl et al. 2008a]. The study showed that worsening of symptoms (interview) was significantly associated with lower levels of self-reported physical activity (International Physical Activity Questionnaire [IPAQ]) in a group of 51 subjects with MS. The study supports symptoms as a possible explanation for the rate of physical inactivity among MS patients but the direction of the cause and effect relationship could still not be established. Based on the results the authors suggest that managing symptoms might be important for the promotion of physical activity, but also that symptoms may be both an antecedent and consequence of physical activity.
After that Motl and colleagues published a cross-sectional study examining the correlation between physical activity and neurological impairment and disability in a group of 80 MS patients [Motl et al. 2008c]. Physical activity (7-day accelerometer day), impairment and disability (Symptom Inventory and self-reported EDSS) was measured and significant correlations were found between physical activity and both EDSS (r = ?0.60) and Symptom Inventory (r = ?0.56). The authors concluded that physical activity was associated with reduced neurological impairment and disability, but also stated that no causal relationship could be established due to the cross-sectional nature of the study.
Motl and McAuley then published a large-scale longitudinal questionnaire study examining the changes in physical activity (Godin Leisure-Time Exercise Questionnaire and 7-day accelerometer data) and symptoms (Symptom Inventory and MS-related Symptom Checklist) as correlates of changes in functional limitations and disability (Late-Life Function and Disability Inventory) [Motl and McAuley, 2009]. A total of 292 MS patients were followed for 6 months. Again a model based on the disablement model proposed by Nagi (1976) was tested as the primary model and this showed that change in physical activity was associated with residual change in function (r = 0.22) and change in function was associated with residual change in disability (r = 0.20). This led the authors to conclude that the findings indicate that change in physical activity is associated with change in disability (through an association with function) consistent with Nagi�s disablement model, but other models may be applied during analysis and a causal interpretation, therefore, still could not be adopted.
In a 6-month longitudinal study Motl and colleagues then tested the hypothesis that a change in physical activity (Godin Leisure-Time Exercise Questionnaire and International Physical Activity Questionnaire) would be inversely associated with a change in walking impairment (Multiple Sclerosis Walking Scale-12) in patients with relapsing�remitting MS [Motl et al. 2011a]. Data from 263 MS patients were analyzed using linear panel analysis and covariance modeling. Findings showed that a standard deviation unit change of 1 in physical activity was associated with a standard deviation unit residual change of 0.16 in walking impairment. These findings, therefore, support physical activity as an important approach, when trying to avoid walking impairments.
Finally, Motl and McAuley published a paper on longitudinal data (6 months) from 292 MS patients evaluating the relationship between a change in physical activity (7-day accelerometer data) and change in disability progression (Patient Determined Disease Steps Scale) [Motl and McAuley, 2011]. Panel analysis showed that a change in physical activity was associated with a change in disability progression (path coefficient: �0.09). This led the authors to conclude that a reduction in physical activity is a behavioral correlate (but not necessarily a cause) of short-term disability progression in persons with MS.
Recently, Tallner and colleagues evaluated the relationship between sports activity (Baecke Questionnaire � sports index) and MS relapses during the last 2 years (based on self-reports) in 632 German MS patients [Tallner et al. 2011]. Patients were divided into four groups based on their sports index. The study showed no overall differences between the four groups concerning the number of relapses within the last 2 years. However, the most active group had the lowermost mean and standard deviation of all groups. Consequently, these data suggest that exercise does not negatively influence relapse rate and the data further indicate that exercise actually reduce relapse rate.
In summary, patient-reported measures of the association between exercise or physical activity and disease progression (expressed as symptoms, functional limitations or disability) or activity (relapse rate) provide evidence of an association with more physical activity providing protection. However, due to the nature of the studies the causality of this association has not been established.
Disease Progression Evaluated in Animal Studies
Some obvious methodological difficulties exists in designing a human study clarifying whether or not exercise has an impact on disease progression in MS patients. Therefore, the question has been addressed in the EAE animal model of MS.
In a preliminary study by Le-Page and colleagues four groups of EAE rats were followed from day 1 to day 10 after injection with an agent inducing EAE [Le-Page et al. 1994]. The injection resulted in three different disease courses in the rats, namely acute (rats rapidly developed serious clinical signs and died without signs of recovery), monophasic (rats developed only one bout of disease followed by complete recovery) and chronic relapsing (CR-EAE, more than one bout of disease followed by remission). The CR-EAE disease course is characterized by the development of an initial acute paralytic attack 10�20 days after immunization with neuroantigens and the development of spontaneous relapses thereafter. A female and a male group of rats exercised and a female and male group served as control. Exercise consisted of running on a treadmill from day 1 to day 10 after injection. The protocol was progressively adjusted with the duration increasing from 60 min towards 120 min and the running speed increasing from 15 to 30 m/min. The study showed that in the exercised CR-EAE rats of both sexes the onset of the disease was significantly delayed compared with the onset in control CR-EAE rats. Also, the duration of the first relapse was significantly reduced in exercised CR-EAE rats compared with control rats whereas no effect was seen on the peak severity of the disease. No effects of exercise were observed in the acute and monophasic EAE rats. The authors concluded that endurance exercise during the phase of induction of EAE diminished lightly one type of EAE (CR-EAE) but also that exercise did not exacerbate the disease.
In a complementary study Le-Page and colleagues conducted further four experiments in the monophasic EAE model [Le-Page et al. 1996]. Experiments 1 and 2 showed that 2 consecutive days of intensive exercise (250�300 min/day) performed just after injection had a lowering effect on the course of the clinical signs of disease as compared with control rats. Also, the onset of the disease and the day of maximal severity were both delayed in the exercising rats, whereas no change was observed in disease duration. When the 2 consecutive days of exercise were performed before injection no effects were observed. In experiments 3 and 4 it was tested how 5 days of more moderate exercise at either constant (15�25 m/min for 2 hours) or variable speed (3 min at 2 m/min and then 2 min at 35 m/min for a total of 1 hour) affected the course of the disease and the clinical parameters. No effects were observed on the disease course and on the clinical parameters. The authors concluded that severe exercise contrary to more moderate exercise slightly influenced the effector phase of monophasic EAE, and confirmed that physical exercise performed before onset of EAE did not exacerbate the clinical signs.
More recently, Rossi and colleagues further explored the effects of physical activity on disease progression in the CR-EAE mice model [Rossi et al. 2009]. In this study one group of mice had their cage equipped with a running wheel on the day of immunization, while the control group had no running wheel. The amount of physical activity was not controlled and it was therefore the amount of voluntary physical activity in the running wheel that constituted the intervention. In a further experiment EAE mice in standard cages were compared with EAE mice in cages equipped with a blocked wheel. This was done to dissect the role of physical activity from that of sensory enrichment caused by the wheel itself, and showed not to influence the clinical course of the disease. During the initial phase (13 days after injection) of the disease the exercising mice ran spontaneously an average of 760 turns/day in the running wheel which dropped to 18 turns/day when motor impairment peaked (20�25 days after injection). The study showed that the severity of EAE-induced clinical disturbances was attenuated in both acute and chronic phases of EAE in the physically active mice, who consistently exhibited less severe neurological deficits compared with control EAE animals during a time period of 50 days after EAE induction. Furthermore, it was shown that both synaptic and dendritic defects caused by EAE were attenuated by physical activity.
In summary, aerobic exercise (or voluntary physical activity) has the potential to influence the clinical course of the disease in the EAE animal model of MS.

Participating in physical activities and exercise can be beneficial for anyone, especially for people with multiple sclerosis, or MS. Exercise can help ease multiple sclerosis symptoms, however, patients have to be careful with the amount of physical activity they engage in. Several research studies like the one discussed in this article have determined that physical activities and exercises can help improve symptoms as well as slow down the progression of multiple sclerosis. It’s essential to talk to a healthcare professional to discuss the details of each workout program in order to make the best of the benefits of exercise for MS. Dr. Alex Jimenez D.C., C.C.S.T.
Discussion
Recent evidence from studies applying nonclinical and patient-reported measures as well as from studies applying the EAE animal model of MS indicate a possible disease-modifying effect of exercise (or physical activity) but the strength of the evidence limits definite conclusions. Furthermore, these findings are not confirmed in intervention studies evaluating disease progression by clinical outcome measures. Despite the obvious associated difficulties future long-term exercise intervention studies in a large group of MS patients are needed within this field.
MS Disease Progression
Some major methodological problems arise when trying to measure MS disease progression. The ideal MS outcome measure would quantify irreversible sustained disease progression, but in MS this has proven difficult. The pleiotropic expression of MS makes it challenging to measure all facets of the disease and it may be necessary to focus on specific symptoms. Furthermore, great patient heterogeneity, population variability in the disease course and tempo of progression, subclinical MRI changes of uncertain impact on delayed disability progression, multifaceted neurological deficits with varied abilities for individual patients to compensate and patient comorbidities complicate things further [Goldman et al. 2010].
Clinical Outcome Measures
EDSS, MSFC and relapse rate are the standard clinical outcome measures for MS therapeutic trials and the most widely used measure of disease progression is the EDSS [Goldman et al. 2010]. Our literature review shows that exercise studies (resistance, endurance and combined training) applying EDSS generally do not report any change after an exercise intervention. In medical studies applying EDSS, large sample sizes and interventions lasting 2�3 years are typically required to measure changes in exacerbation rates between treatment and placebo [Bates, 2011]. This corresponds poorly to the short intervention periods (3�26 weeks) and the small sample sizes applied in most exercise studies. This is due to the overall low responsiveness and sensitivity to change of the EDSS as reported in a number of studies (for references see Goldman et al. [2010]). Also, the EDSS have been criticized for its noninterval scaling, emphasis on ambulation status and absence of adequate cognitive and visual components [Balcer, 2001]. Despite the emphasis on ambulation and that a recent meta-analysis concluded that exercise impacts walking positively [Snook and Motl, 2009], no changes were seen in the EDSS in most of the reviewed studies, indicating low scale responsiveness towards exercise interventions. In clinical trials the MSFC is claimed to be more sensitive to change than the EDSS [Goldman et al. 2010]. This suggestion is supported by the finding from one exercise study applying both the EDSS and the MSFC. In this long-term study (26 weeks) [Romberg et al. 2005] the effects of combined training on EDSS and MSFC were evaluated. Only the MSFC showed a significant effect which led the authors to conclude that the MSFC was more sensitive than the EDSS in the detection of improvement of functional impairment as a result of combined exercise. In future exercise studies evaluating disease progression it should therefore be considered to add the MSFC as a clinical outcome measure.
In addition to low scale responsiveness, short-term interventions and small sample sizes other explanations for the general lack of effects on clinical outcome measures can be hypothesized. Despite no clear pattern in the existing data, the type of exercise (e.g. endurance versus resistance training) may influence the effect captured by clinical scales. Also, most studies have evaluated mild to moderately impaired (EDSS <6) MS patients. Perhaps the clinical scales would be more sensitive to change in more severely impaired patients. Finally, findings can be biased if it is generally more physically fit patients that accept to be enrolled in exercise studies. If so, the baseline fitness level may be above average in these patients further lowering the possibility of a change on clinical scales with low responsiveness.
Only a few studies [Bjarnadottir et al. 2007; Petajan et al. 1996; Romberg et al. 2004; White et al. 2004] present clear data on relapse rate but due to the short intervention periods and the small sample sizes in most studies changes in the relapse rate, would not be expected to be evident. However, Romberg and colleagues found a total of 11 relapses (five in the combined training group and six in the control group) during a 6-month intervention period [Romberg et al. 2004]. Similarly, Petajan and colleagues (endurance training group four relapses and control group three relapses) [Petajan et al. 1996] and Bjarnadottir and colleagues (combined training group one relapse and control group one relapse) [Bjarnadottir et al. 2007] reported identical relapse rates in exercise and control groups. In the study by White and colleagues no participants experienced relapses during the 8-week intervention evaluating resistance training [White et al. 2004]. Recently, Tallner and colleagues collected self-report questionnaires on relapse rates and physical activity from MS patients to examine the relationship of different levels of sports activity and relapses [Tallner et al. 2011]. Based on these data the authors concluded that exercise had no significant influence on clinical disease activity. Taken together the few existing data do not indicate that any type of exercise increases relapse rate among MS patients. However, these data should be interpreted with caution due to the small number of participants (not stratified according to disease type or severity) and the short intervention periods in most studies. Consequently, future long-term studies with a large number of participants should, therefore, include relapse rate as an outcome measure.
Nonclinical Measures
Application of MRI has revolutionized the diagnosis and management of patients with MS [Bar-Zohar et al. 2008]. In regard to clinical trials, MRI offers several advantages over the accepted clinical outcome measures for MS, including an increased sensitivity to disease activity and a better association with histopathology findings. Also, MRI provides highly reproducible measures on ordinal scales, and the assessment of MRI can be performed at the highest degree of blinding [Bar-Zohar et al. 2008]. Consequently, a surrogate MRI measure reflecting disease progression such as lesion activity (gadolinium-enhanced lesions and new or enlarged T2-hyperintense lesions) or disease severity (total T2-hyperintense lesion volume, total T1-hypointense lesion volume and whole-brain atrophy) [Bermel et al. 2008] may reduce the required sample sizes needed to evaluate the effects of exercise therapy on disease progression considerably. Until now only two cross-sectional studies have evaluated the effects of exercise (expressed as the current cardiorespiratory fitness level) on different MRI measures limiting the conclusions that can be drawn from this type of study. However, the promising findings do encourage the inclusion of MRI as an outcome measure, in future longitudinal trials evaluating the effects of exercise on disease progression.
Patient-Reported Measures
Patient-reported measures of the association between exercise or physical activity and disease progression (expressed as symptoms, functional limitations or disability) provide evidence of an association with more physical activity providing protection. However, the nature of the studies does not allow conclusions on the causality of this association. In the group of studies applying patient-reported measures we decided to include not only measures of exercise, but also measures of physical activity. It is acknowledged that a measure of physical activity is not necessarily a surrogate measure of exercise, but the many interesting findings from particularly the group of Motl and colleagues caused this. In a recent paper, based on their own studies, Motl and colleagues concludes that recent research has identified physical activity as a behavioral correlate of disability in MS. This made the authors suggest, that physical activity might attenuate the progression of what they call �mobility disability� by improving physiological function in persons with MS, particularly those who have achieved a benchmark of irreversible disability (EDSS >4) [Motl, 2010]. It might be more cost effective to offer the more disabled (EDSS >4) MS patients exercise therapy, but it must be noted that most exercise studies do not indicate that a relationship between the degree of training adaptation and neurological disability exist. In fact, studies indicate that MS patients with an EDSS score below 4.5 experience the largest improvements after a period of endurance training as compared with more disabled MS patients [Ponichtera-Mulcare et al. 1997; Schapiro et al. 1988] or that no differences exists [Petajan et al. 1996]. It must be noted that none of these studies were powered to evaluate the effects of exercise in MS patients with different levels of disability. However, a recent study by Filipi and colleagues specifically evaluated whether 6 months of resistance training improves strength in MS patients with different levels of disability (EDSS 1�8) and concluded that all individuals with MS, despite different disability levels, showed parallel improvement in muscle strength [Filipi et al. 2011]. This leads to the suggestion, that exercise may be equally important during the early phases of the disease, also in regard to impact on disease progression.
An important advantage of applying patient-reported measures is the opportunity to collect data from large sample sizes in longitudinal studies. Furthermore, it seems important to collect data on patient perspective when evaluating the effects of exercise on disease progression. Future studies including patient-reported measures should also include clinical and/or nonclinical outcome measures if possible.
Animal Studies
Our review showed that aerobic exercise (or activities) has the potential to influence the clinical course of the disease in the EAE animal model of MS. The obvious question is whether or not the findings from the EAE animal model of MS can be extrapolated to humans. At the moment no clear answer can be given to this question. A recent review summarized whether the current disease-modifying treatments are justified on the basis of the results of EAE studies. Here it was concluded that although EAE is certainly an imperfect mirror of MS, many clinical, immunopathological and histological findings are impressively replicated by animal models, making EAE invaluable in elucidating the basic immunopathological mechanisms of MS and providing a testing ground for novel therapies [Farooqi et al. 2010]. Consequently, a direct transfer of findings into human subjects cannot be made, but testing of difficult hypotheses can start here. Also, it should be noted that in EAE you cannot control the relative exercise intensity since no maximal exercise test (such as a VO2 max test) can be performed. As a consequence the applied relative exercise intensity may differ between animals. This is also why it is very difficult to evaluate the effects of aerobic exercise on aerobic capacity in EAE. Nonetheless, the EAE model offers a number of advantages compared to human studies. In addition lower costs, easy control with adherence to the intervention and controlled environmental and genetic factors the EAE model also allows evaluation of possible mechanisms located in the central nervous system (CNS), which should have attention in future studies. Another review stated that the genetic heterogeneity, which is so critical in the MS population, is only reflected when multiple different models of EAE are studied in parallel [Gold et al. 2006]. This aspect should also be incorporated in future studies.
Possible Mechanisms
Several mechanisms have been proposed as a possible link between exercise and disease status in MS. Some of the most promising candidates include cytokines and neurotrophic factors [White and Castellano, 2008a].
Cytokines. Cytokines play an important role in the pathogenesis of MS and are a major target for treatment interventions. In particular, interleukin (IL)-6, interferon (IFN)-? and tumor necrosis factor (TNF)-? have a prominent role in the process of demyelination and axonal damage experienced by persons with MS [Compston and Coles, 2008].
Changes in the concentrations of certain cytokines, in particular IFN-? and TNF-?, have been associated with changes in disease status in MS, and elevated concentrations of pro-inflammatory Th-1 cytokines (such as TNF-?, IFN-?, IL-2 and IL-12) may contribute to neurodegeneration and disability [Ozenci et al. 2002]. This has led to the suggestion that exercise may counteract imbalances between the pro-inflammatory Th1 cytokines and the anti-inflammatory Th2 cytokines (such as IL-4 and IL-10) by enhancing anti-inflammatory mechanisms, and thereby potentially be able to alter the disease activity in MS patients [White and Castellano, 2008b].
In MS both the acute and/or chronic effects of resistance [White et al. 2006], endurance [Castellano et al. 2008; Heesen et al. 2003; Schulz et al. 2004] and combined training [Golzari et al. 2010] on several cytokines have been evaluated. A study by White and colleagues reported that resting levels of IL-4, IL-10, C-reactive protein (CRP) and IFN-? were reduced, while TNF-?, IL-2 and IL-6 levels remained unchanged after 8 weeks of biweekly resistance training [White et al. 2006]. These results suggest that progressive resistance training may have an impact on resting cytokine concentrations and, thus, could have an impact on overall immune function and disease course in individuals with MS. However, the study was not controlled and only 10 participants were included obviously limiting the strength of the evidence. Heesen and colleagues evaluated the acute effects of 8 weeks of endurance training on IFN-?, TNF-? and IL-10 and compared this to both a waitlist MS control group and a group of matched healthy subjects [Heesen et al. 2003]. After completing 30 minutes of endurance training (cycling) an increase in IFN-? were induced similarly in all groups while trends towards smaller increases in TNF-? and IL-10 were observed in the two groups of MS patients. Based on these data the authors concluded, that no deviation in pro-inflammatory immune response to physical stress could be demonstrated in MS patients. These findings, therefore, supports that a single bout of endurance training can influence the cytokine profile at least for a period of time in MS patients. In another publication from the same study Schulz and colleagues were not able to demonstrate any differences between the resting level or the acute IL-6 response after 30 minutes of endurance exercise in the MS training group (8 weeks of bicycling) and the MS control group [Schulz et al. 2004].
A study by Castellano and colleagues evaluated the effects of 8 weeks of endurance training (cycling, 3 days/week) on IL-6, TNF-? and IFN-? in 11 MS patients and 11 healthy matched controls. In MS patients both resting IFN-? and TNF-? was elevated after endurance training whereas no changes were observed in healthy controls [Castellano et al. 2008]. Like in the study by Heesen and colleagues [Heesen et al. 2003], Castellano and colleagues also studied the acute effects of a single bout of endurance training and similarly found no differences when compared to the healthy controls, but in this study no increase in IFN-? and TNF-? were observed in any of the groups contrasting the findings by Heesen and colleagues.
In the most recent study Golzari and colleagues performed a randomized controlled trial (RCT) evaluating the effects of 8 weeks of combined endurance and resistance training on IFN-?, IL-4 and IL-17 [Golzari et al. 2010]. The study showed significant reductions in the resting concentrations of IFN-? and IL-17 in the exercise group, whereas no changes were seen in the control group, but no group comparisons were made.
In summary, no clear pattern can be seen in the reported cytokine responses to exercise probably reflecting large methodological differences between the studies (study type, type of exercise intervention, time of measurements, standardizations, etc.) and a low statistical power which is critical due to the great variation in this type of measurements. Nonetheless, a single bout of exercise have been reported to influence a number of (pro-inflammatory) cytokines in MS patients and also chronic changes in the resting concentration of several cytokines have been reported after a training period. Furthermore, the response seems to be comparable to that of healthy subjects. Cytokines, therefore, may link exercise and disease progression in MS, but large-scale future RCTs have to evaluate this further.
Neurotrophic factors. Neurotrophic factors are a family of proteins that are thought to play a role in preventing neural death and in favoring the recovery process, neural regeneration and remyelination throughout life [Ebadi et al. 1997]. Some of the more well-characterized neurotrophic factors include brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF) [White and Castellano, 2008b].
Gold and colleagues evaluated the acute effects of a single exercise bout (30 min cycling at 60% VO2 max) on NGF and BDNF in 25 MS patients and compared this with a group of matched healthy controls [Gold et al. 2003]. The study showed that baseline concentrations of NGF were significantly higher in MS patients compared with controls. Thirty minutes after exercise a significant increase was observed in BDNF while a trend towards an increase in NGF was observed. However, the changes did not differ from the changes observed in the healthy subjects. This made the authors conclude that moderate exercise can be used to induce neutrophin production in subjects with MS possibly mediating the beneficial effects of physical exercise. In a study from the same group Schulz and colleagues evaluated the effects of biweekly cycling for 8 weeks on BDNF and NGF in a RCT in MS patients [Schulz et al. 2004]. The study showed no effects on the resting concentration and on the response to acute exercise after the intervention period, and only a trend towards lower resting NGF levels was found. Castellano and White also evaluated whether 8 weeks of cycling (three times a week), would affect serum concentrations of BDNF in MS patients and in healthy controls [Castellano and White, 2008]. In contrast to the findings of Gold and colleagues, resting BDNF was lower at baseline in MS patients as compared with controls, but no difference (a trend) between groups was found after 8 weeks. In MS patients BDNF concentration at rest was significantly elevated between weeks 0 and 4 and then tended to decrease between weeks 4 and 8, whereas resting BDNF concentration remained unchanged at 4 and 8 weeks of training in controls. Also, the response to a single bout of exercise was evaluated showing a significant reduction in BDNF 2 and 3 hours after exercise in both groups again contrasting with the findings by Gold and colleagues. The authors concluded that their findings provided preliminary evidence showing that exercise may influence BDNF regulation in humans.
In summary contrasting findings on the effects of exercise on neurotrophic factors exists in MS patients, making more studies warranted. However, findings do imply that exercise may influence several neurotrophic factors known to be involved in neuroprotective processes.
Conclusions
It cannot be clearly stated whether exercise has a disease-modifying effect or not in MS patients but studies indicating this do exist. Future long-term intervention studies in a large group of MS patients are therefore needed to address this important question.
Acknowledgments
The authors would like to thank research Librarian Edith Clausen for a substantial contribution to the comprehensive literature search.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
UD has received travel grants and/or honorary from Biogen Idec, Merck Serono and Sanofi Aventis. ES has received research support and travel grants from Biogen Idec, Merck Serono and Bayer Schering and travel grants from Sanofi Aventis.
Multiple sclerosis, or MS, is a chronic disease identified by symptoms of by pain, fatigue, vision loss and impaired coordination caused by damage to the myelin sheaths of nerve cells in the central nervous system, or CNS. Exercise has been demonstrated to help improve the management of symptoms of multiple sclerosis as well as decrease the progression of the disease, although further evidence is still required, the article above summarizes these outcome measures. The purpose of the article above demonstrates how exercise can change the progression of multiple sclerosis and improve overall health and wellness. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Referenced from: Ncbi.nlm.nih.gov/pmc/articles/PMC3302199/

Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �

EXTRA EXTRA | IMPORTANT TOPIC: Recommended El Paso, TX Chiropractor
***
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Exercise and Disease Progression in Multiple Sclerosis" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933






