
El Paso, TX. science based chiropractor, Dr. Alexander Jimenez looks at this uncommon problem � and how it can be treated.
The true incidence of obturator externus accidents is unknown, as frequently they may be misdiagnosed as hip joint pathology and/ or groin pathology as the website of symptoms as well as also the presenting objective signals may mimic other pathologies such as hip joint labrum pathology, anterior femoral triangle issues and perhaps even gluteal pathology.
Injury for this muscle gifts as a deep obscure groin/hip pain and functionally the muscle may still hide direct involvement as a pain generator since it is primarily a equilibrium muscle rather than a force-producing hip muscle.
This case study presents an unusual case of hip-related pain in a professional baseball player which also shown itself as an injury to the contralateral adductor longus.
Contents
The Player
As he was wrestled to the floor, his right hip was compelled at a rapid and loaded flexion/internal turning position. His first sensation was pain deep inside the anterior hip/groin area.
When he presented to the medical team with the accident, he complained of a profound catching sensation inside the hip joint location. It had been difficult to fully bend the hip and to also twist on the stationary limb (because he did whilst kicking a ball). His prior background consisted of a right-sided inguinal hernia repair five seasons before as well as a few gentle on again/off back osteitis pubis-type signs that would normally flare from the first period as his goal-kicking amounts have been increased. He was obviously a left- footed goal kicker.
On examination, he observed that the pain to become worse on passive flexion/internal rotation of the hip (hip walkway test). He was noticeably tight and irritated from the shallow TFL muscle, and also posteriorly across the greater trochanter around the insertion for the gluteals and deep hip rotators. He was also particularly high tone in the right iliopsoas muscle.
He was initially diagnosed clinically because of hip joint sprain due to the mechanism of harm being a pressured flexion/internal rotation type position that would always put pressure on the anterior hip joint capsule/labrum.
He was treated initially with deep iliopoas muscle sparks and hip joint mobilizations using a seat belt to gap the hip joint. He reacted reasonably well with the therapy and immediately felt more comfortable on a hip joint quadrant test. He was rested from coaching for 2 days and ran on the next day and played a match on the fourth day. But during the match, though his right hip did not create any pain, he’d notice pain on his left adductor source that was more pronounced during kicking.
Three days post-game he detected this ongoing left adductor origin pain and it was made worse by kicking again through training. An MRI was performed to Look at the left adductor origin and also the report noted:
- Grade 1 left adductor longus strain deep in the
- Grade 2 right obturator externus strain on its femoral attachment
- Grade 1 right iliopsoas muscle strain in the MTJ.
The surprise finding on the MRI of a grade 2 obturator strain prompted the medical team to more formally assess the participant for ongoing hip joint disorder. The particular features to notice from this medical examination were:
Subjective
? A sensation of weakness and instability in the right hip whilst kicking with the left foot.
? No pain in the right hip with running, even with top-end speed. However, the left adductor longus was symptomatic on running and kicking.
Objective
? Pain on passive right hip internal rotation whilst in 90-degree hip flexion. This pain was deep anteriorly in the hip, almost presented as a groin problem.
? Some discomfort on resisted right hip flexion/external rotation deep inside the iliac fossa.
? Pain and weakness in the left adductor on adductor squeeze tests. These squeeze tests performed at 0/45/90 degrees of knee flexion with a pressure cuff between the knees. Usual pre-season scores measured 260/260/250. On current testing they measured 150/170/180. Pain was felt at the end of the squeeze.
? Discomfort with prone lie hip passive internal rotation. This pain was more focused around the right greater trochanter posteriorly.
Pathomechanics
It had been suspected that this player had endured a secondary injury to the left adductor longus (a muscle used a lot in goal-kicking) due to the inherent failure in bolstering the proper hip throughout the plant phase of the kick due to the inhibition of the right obturator externus, a muscle considered to be an important hip stabilizer and turning control muscle at the hip. With insufficient hip stabilization in kicking, the left hip was required to create more power to compensate for the unstable right hip to gain the length from the kick. Then the left adductor longus failed along with a strain injury led.
Management
The management of the matter initially centered on the two key features being the left-sided adductor strain and the right- sided obturator externus strain.
In the week following the accident, the player was sent to get a series of Actovegin shots to the left adductor longus. This was done according to protocol that was three injections every 48 hours — Monday/ Wednesday/Friday. In this five-day period the adductor longus was handled with deep tissue flush massage and gentle isometric adduction exercises at supine (chunk squeezes) in the three positions of examining — 0/45/90 levels of knee flexion — also as wall squat adductor squeezes in the same positions. The obturator externus was medicated with heavy tissue releases (obtained through the anterior groin region) and direct theraband strengthening of hip external rotation in sitting and in prone. Actovegin shots to the obturator externus are regarded as difficult because of problems with accessing this muscle through the superficial hip musculature.
The adductor exercises progressed into through array adduction with theraband resistance (equally with the left leg being the motion leg as well as the stability leg).
By 12 days post-injury it had been detected that the obturator externus strength had not improved and the player still had deep- seated right back pain pain. It was rationalised that perhaps the direct treatment to this muscle and also the direct open kinetic chain strengthening was possibly making the muscle texture worse. The choice was made to stop any direct hands-on therapy to the muscle and also to prevent any direct open kinetic chain strengthening. Instead the player lasted with bilateral theraband exercises of both hips into flexion and then abduction and expansion in addition to adduction. The avoidance of lead obturator externus soft tissue treatment and exercise appeared to improve the hip function immediately.
The participant started running 20 times post-injury and quickly progressed through running stages over a five-day period of conducting on alternate days. At this point the player’s adductor squeeze scores had improved to steps according to pre- season baselines. However, daily the player ran direct adductor strength operate using a Pilates reformer as a slider drill to immediately load into adduction in addition to hammering theraband adduction exercises in standing and in supine lying.
By 27 days post-injury the player managed to begin kicking, change in direction and rugby training. He played at 30 times post-injury with no ill effects.
Discussion
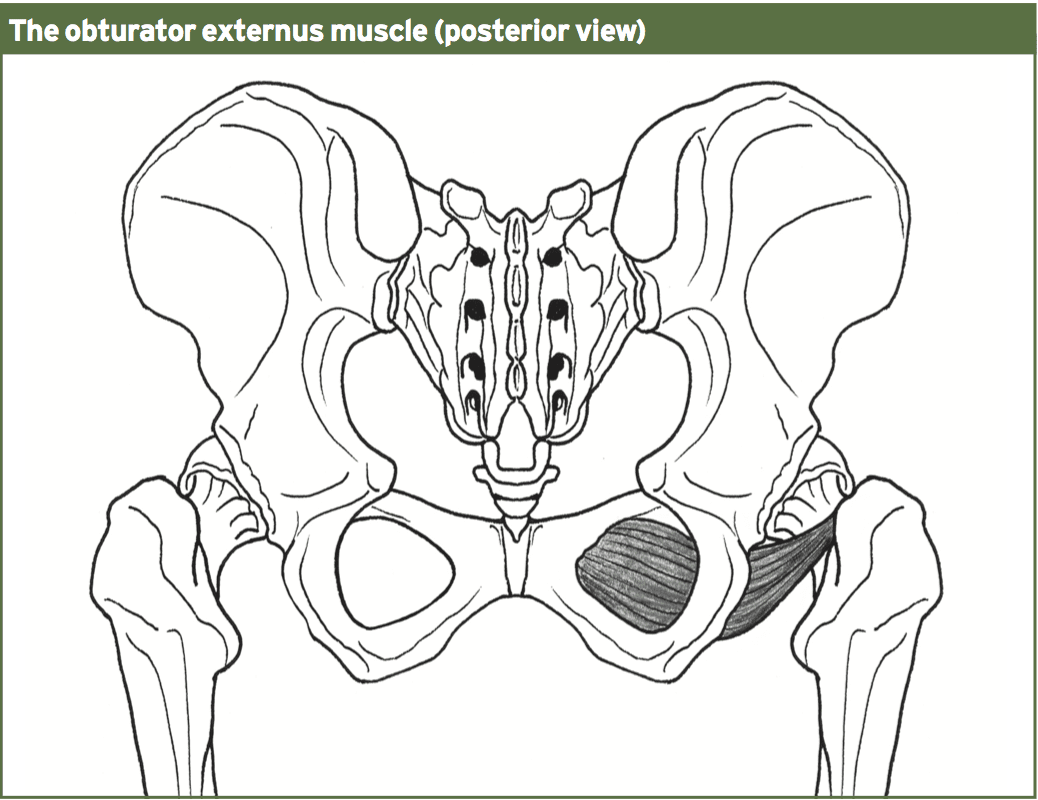
It arises immediately around the medial side of the obturator foramen, as well as the inferior ramus of the ischium; it also arises in the lateral two-thirds of this outer surface of the obturator membrane, and also in the tendinous arch which completes the canal to the passage of the obturator nerves and vessels.
The action of the muscle is to externally rotate the hip and also helps in hip adduction. It’s postulated to also work as a hip balance muscle in one legged stance along with the obturator internus, quadrutus femoris, piriformis and the gemelli muscles. In a practical activity such as kicking, the muscle acts to stabilize or hold the ball of the femur into the socket (acetabulum).
The incidence of harm to the obturator externus muscle is unknown because there are only a handful of case reports from the medical literature that highlight injuries for this muscle. Additionally, among the vexing issues is the difficulty in creating the correct clinical diagnosis based on the history and physical evaluation. MRI imaging is needed to correctly picture injuries to this muscle.
From the case study introduced, injury for the muscle was a direct result of forceful flexion/internal rotation mechanism to the hip joint. As the muscle primarily functions as a hip stabilizer during jogging, it is possible that a patient can mask symptoms during functioning as the muscle isn’t required to produce any hip skate for locomotion.
Nonetheless, in this event the muscle has a role in stability of the hip during kicking, and for that reason may have produced a poor pelvic/hip complicated during kicking that then led to an accident to the adductor longus on the other hand.
In addition, it seems that direct treatment to the muscle in the form of deep trigger point releases and also direct strengthening may actually delay healing in the muscle in case of injury. This may highlight the value of the muscle as a hip stabilizer instead of a legitimate torque manufacturer in hip rotation.
Professional Scope of Practice *
The information herein on "Obturator Externus Injury: Unusual Cause Of Hip/Groin Pain" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Our information scope is limited to Chiropractic, musculoskeletal, physical medicines, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somatovisceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and/or functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez, DC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, RN*, CCST, IFMCP*, CIFM*, ATN*
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807, New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Florida
Florida License RN License # RN9617241 (Control No. 3558029)
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Dr. Alex Jimenez DC, MSACP, RN* CIFM*, IFMCP*, ATN*, CCST
My Digital Business Card





