
Imaging Diagnosis Management:
- Cervical spinal trauma & radiographic variants simulating disease
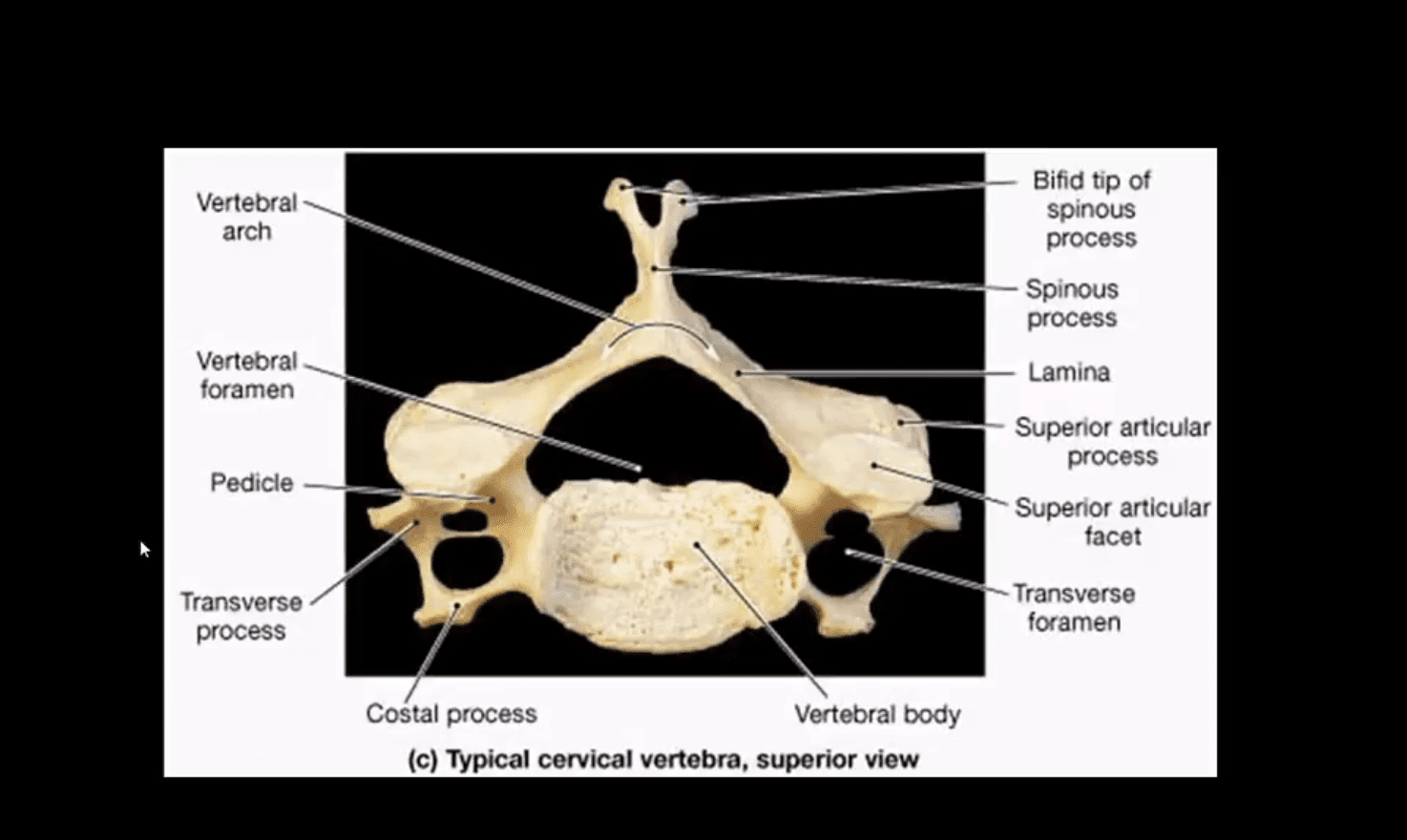
- Cervical spine
- Arthritis
- Neoplasms
- Infection
- Post-Surgical cervical spine
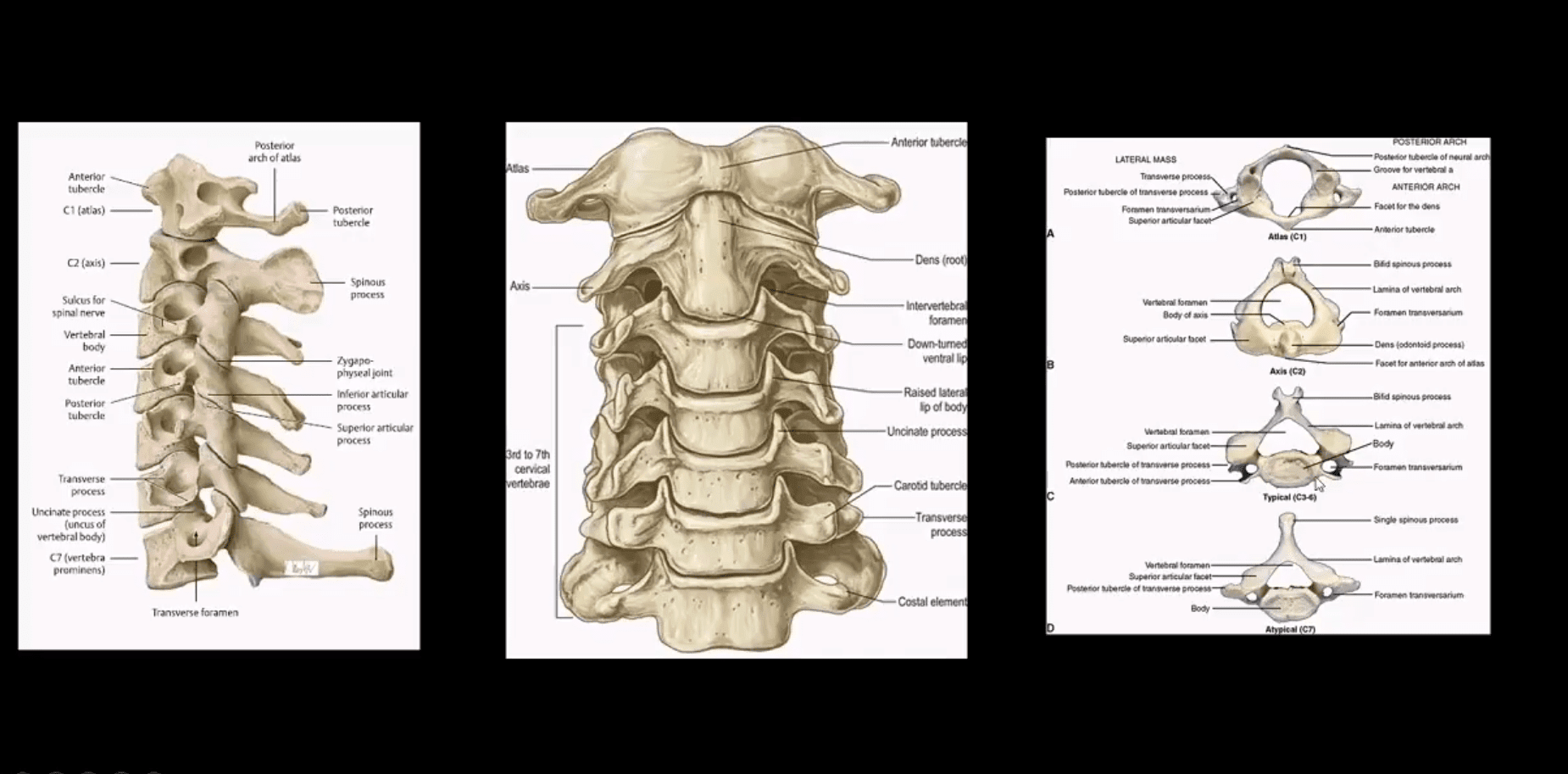
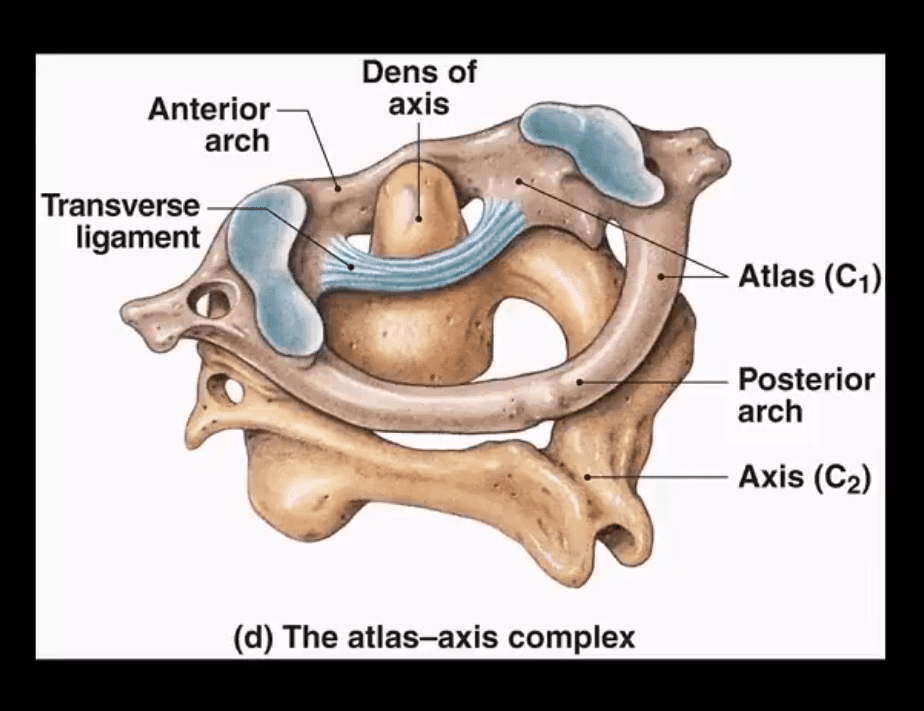
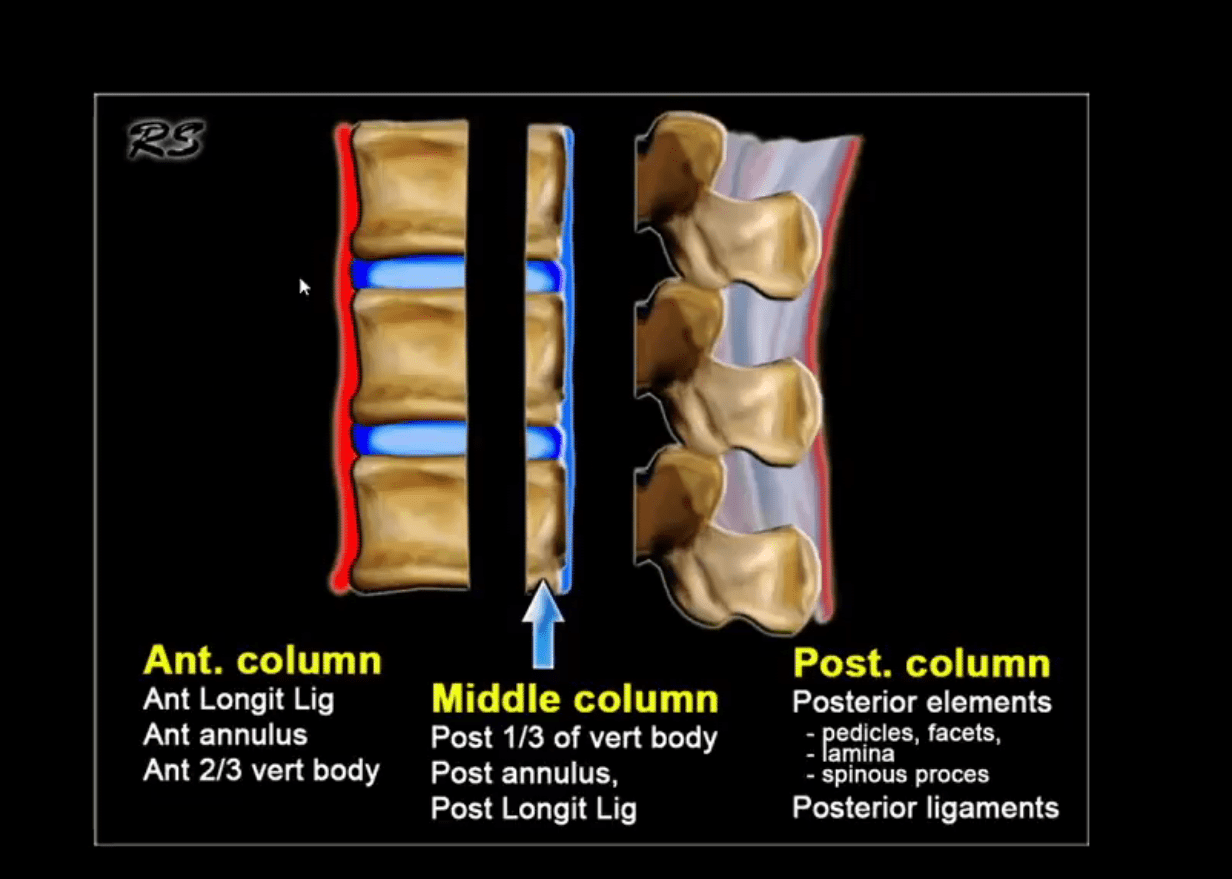
- Cranio-cervical and upper cervical stability is dependent on transverse, superior and inferior bands of the C1-C2 ligament, alar ligaments, along with a few other ligaments
Contents
Cervical Trauma
- The C/S is vulnerable to injury. Why?
- Stability has been sacrificed for greater mobility
- Cervical vertebrae are small and interrupted by multiple foraminae
- The head is disproportionately heavy and acts as an abnormal lever especially when forces act against a rigid torso
- Additionally, C/S is prone to degeneration which makes it more vulnerable to trauma
- In young children, ligaments are more luxed vs. disproportionately large head size
- In children, the fulcrum of movement is at C2/3 thus making injuries more common in the upper C/S and craniocervical junction. In children, S.C.I.W.O.R.A. may occur when no evidence of fracture present
- In adults, the fulcrum of movement is at C5/6 thus making lower C/S more vulnerable to trauma especially during extremes of flexion
- Cervical Trauma categorized according to mechanisms of injury (Harris & Mirvis classification)
Hyperflexion Injury: Stable vs. Unstable
- Flexion teardrop Fx (most severe fracture, unstable)
- Bilateral facet dislocation (severe injury w/o fracture, unstable)
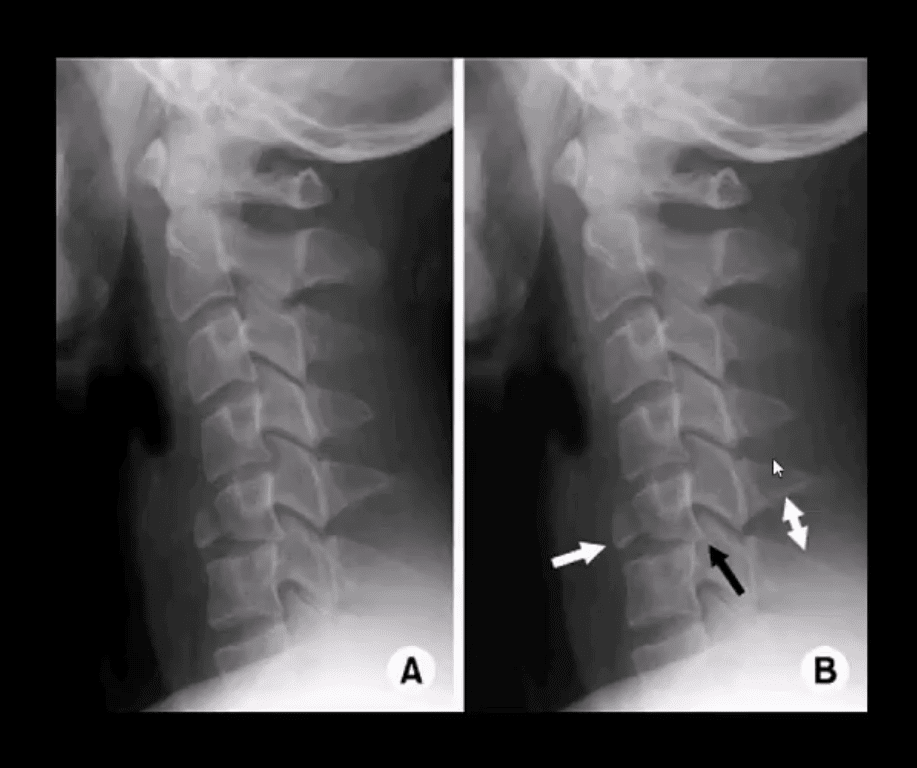
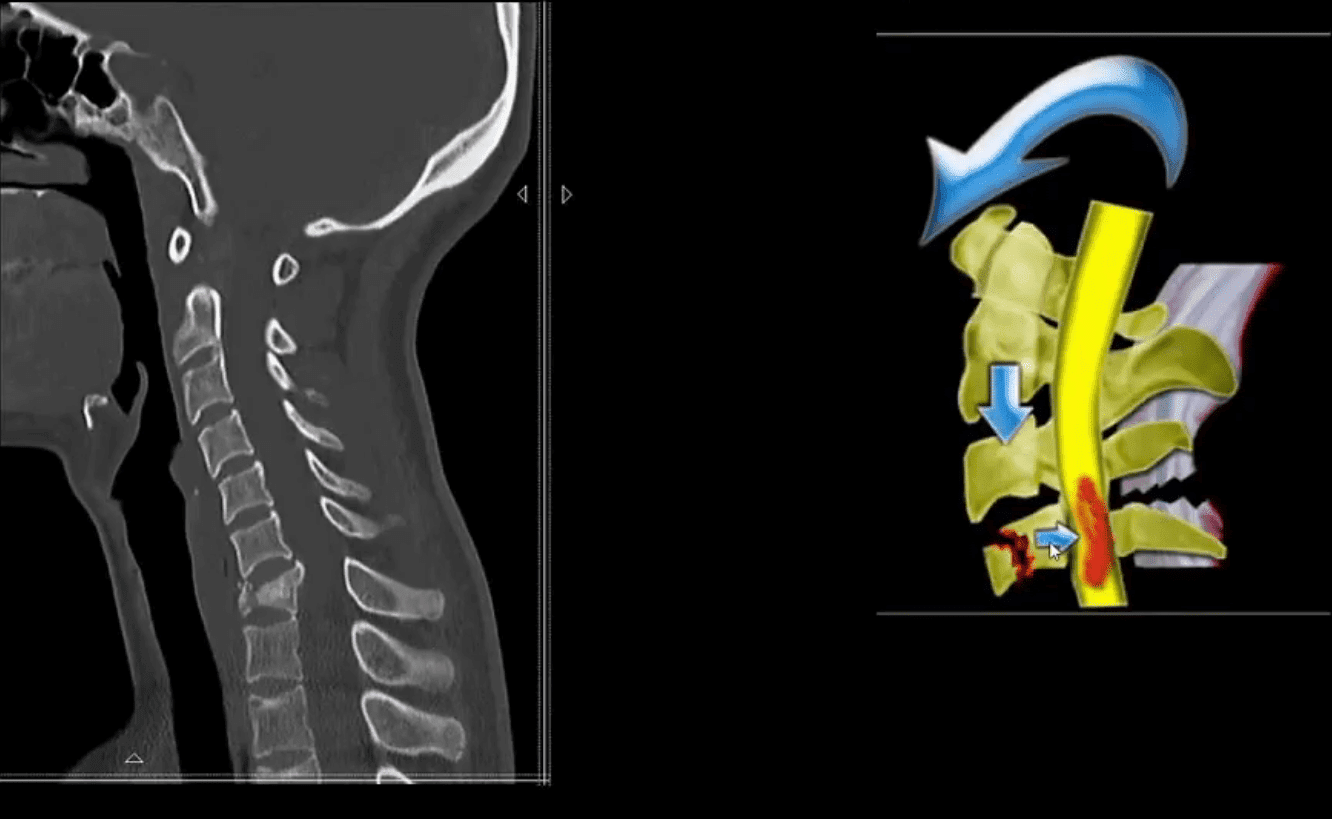
- Anterior subluxation (potentially unstable) can be very subtle injury
- Clay Shoveller Fx (lower C/S SP avulsion, stable)
- Simple wedge compression (most benign Fx, stable)
- Hyperflexion-rotation with unilateral facet dislocation
- Obtain a thorough history
- Perform physical exam including a neurological exam
- Consider NEXUS criteria (National Emergency X-radiography Utilization Study)
Imaging Techniques:
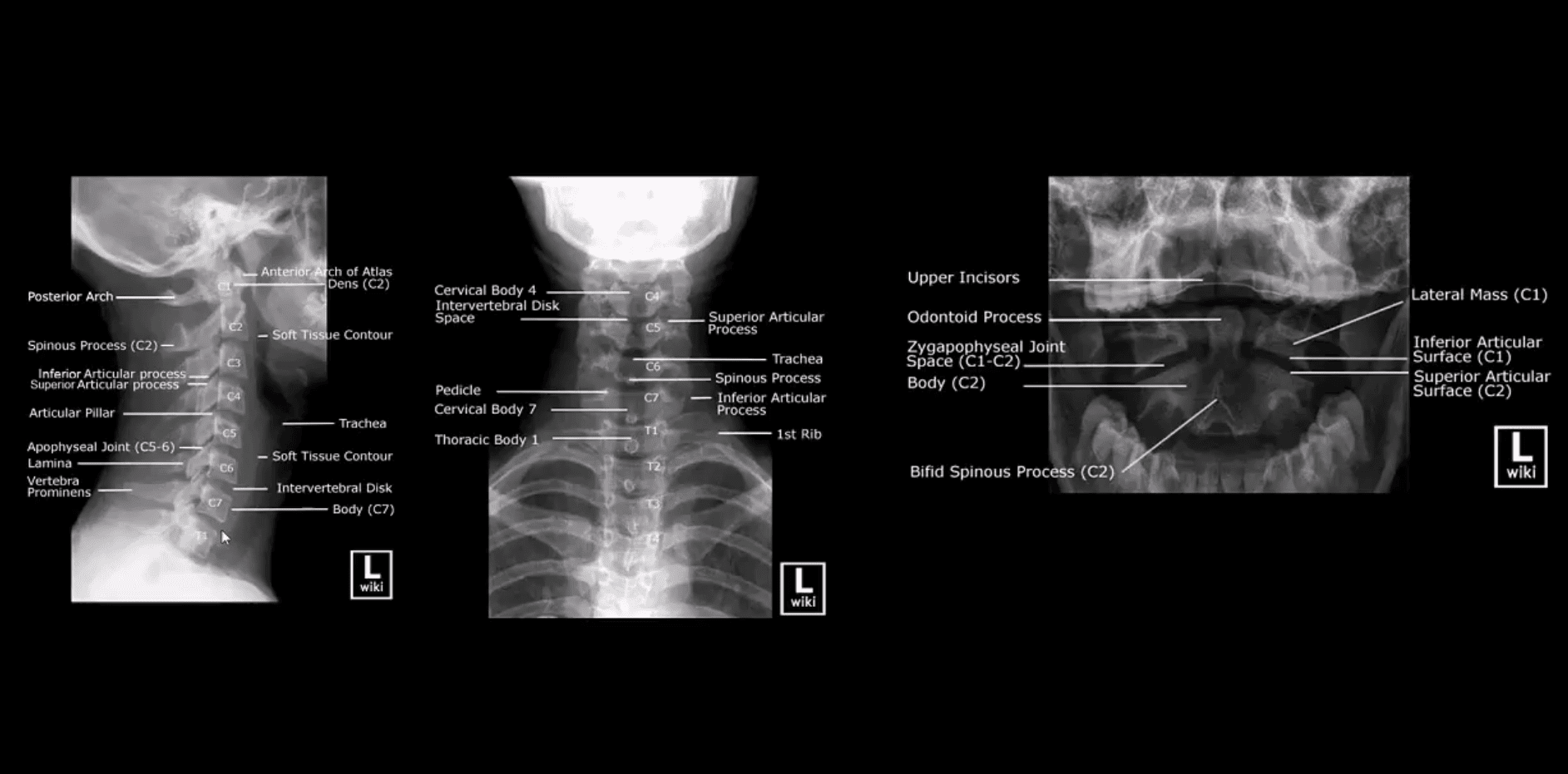
- Begins with x-radiography especially in cases with no significant neurological compromise
- Clear neutral lateral view first
- If x-radiography is unrewarding but high probability of severe trauma and neurological deficit present, CT scanning w/o contrast is required
- Consider CT scanning in patients with pre-existing changes: advance spondylosis, DISH, AS, RA, post-surgical spine, congenital abnormalities (Klippel-Feil syndrome, etc.)
Vertical compression:
- Jefferson aka burst Atlas Fx (unstable especially if the Transverse ligament is torn, cord paralysis in 20-30% only)
- Why? Due to fragments dissociation and canal widening
- Burst Fx of the Thoracic or Lumbar spine (unstable, cord paralysis may occur)
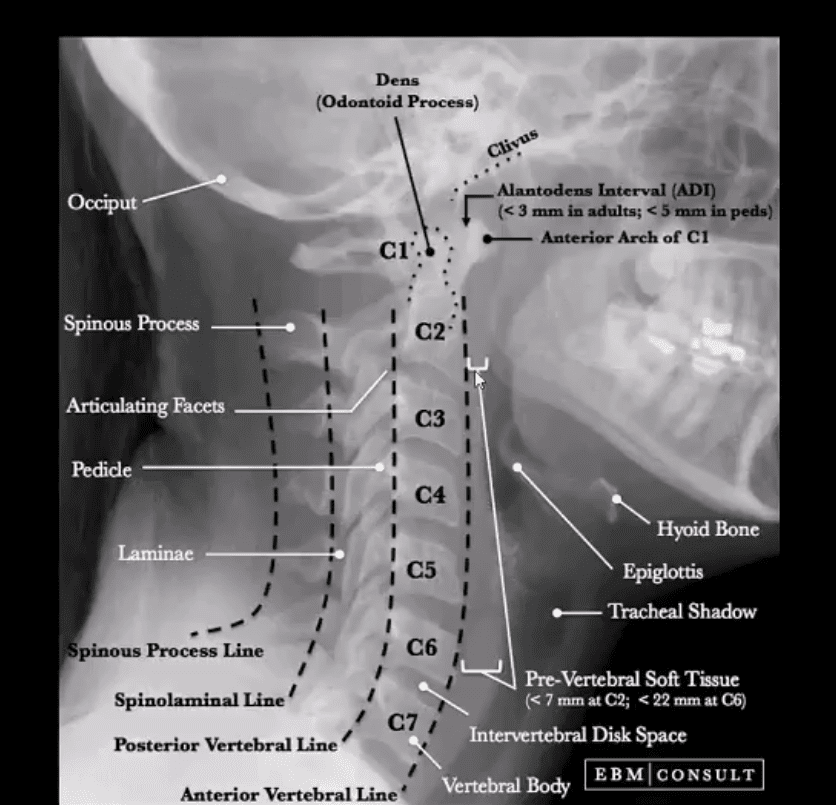
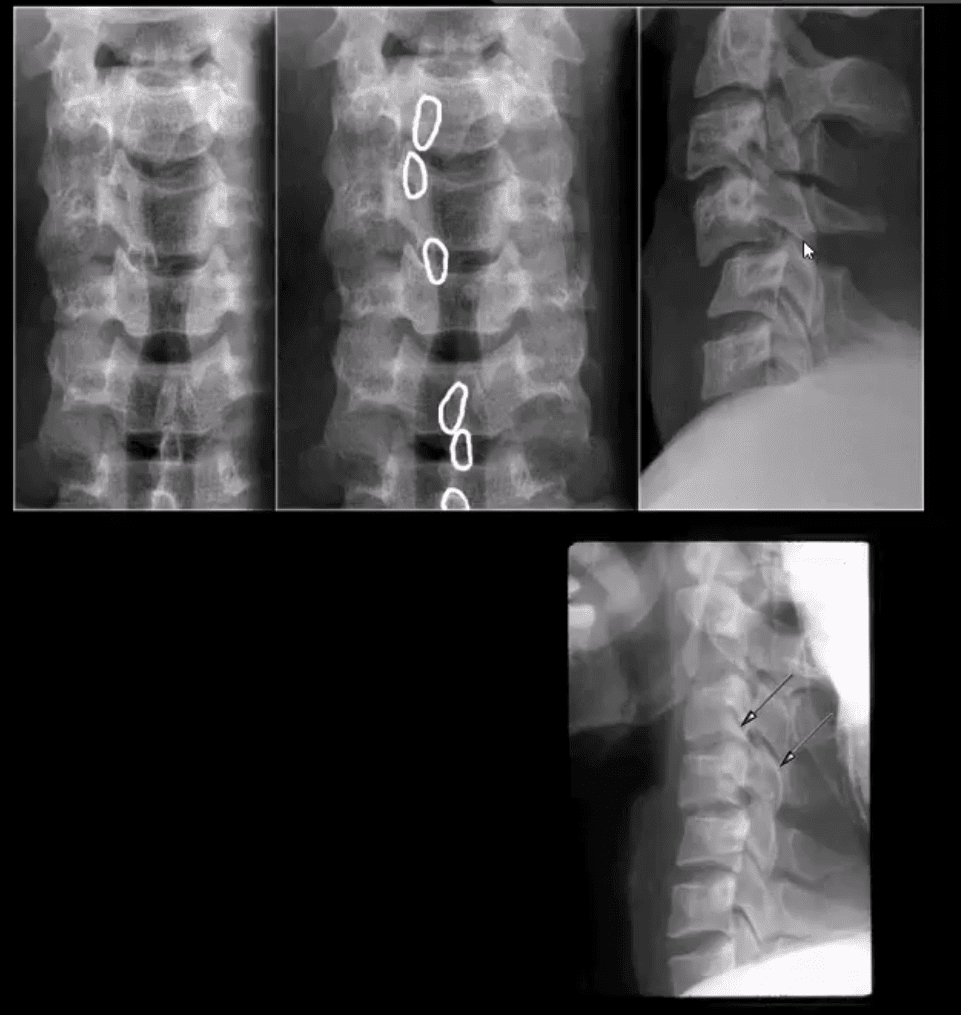
How to Assess Spinal Radiographs in Trauma Cases:
- Construct 5-lines on the lateral view
- Note if facets are well-aligned and symmetrical
- Ensure symmetry of the disc height
- Note any widening or fanning of the inter-spinous distance
- Carefully examine prevertebral soft tissues
- Evaluate atlanto-dental interval (ADI)
- In cases of trauma, evaluate and clear neutral lateral first
- Do not perform flexed and extended views in acute cases before x-rays or CT scanning exclude significant instability
- Pay extra attention to prevertebral soft tissues
- If thicker than normal limits, consider severe post-traumatic bleed
- Subtle asymmetry and widening of posterior disc height and facets with inter-spinous fanning may be a key feature of significant tearing of posterior ligaments
Hyperflexion Injuries (M/C Mechanism)
- More frequent in sub-axial C/S C-3-C7)
- Unstable injuries:
- Flexion teardrop fracture (M/C C5 & C6) v. unstable
- Key rad features:
- Large “teardrop” triangular anterior body fragment
- Fanning of the SPs, posterior disc and facet widening indicating tearing of major spinal ligaments and instability
- A posterior shift of the vertebral body fracture suggests direct anterior cord/vessels compression
- Bulging prevertebral soft tissue >20-mm at C6-7
- 80% of cases may be paralyzed on the spot or develop significant paralysis soon after
Acute Neck Trauma. What are the vital radiographic features? What is the diagnosis?
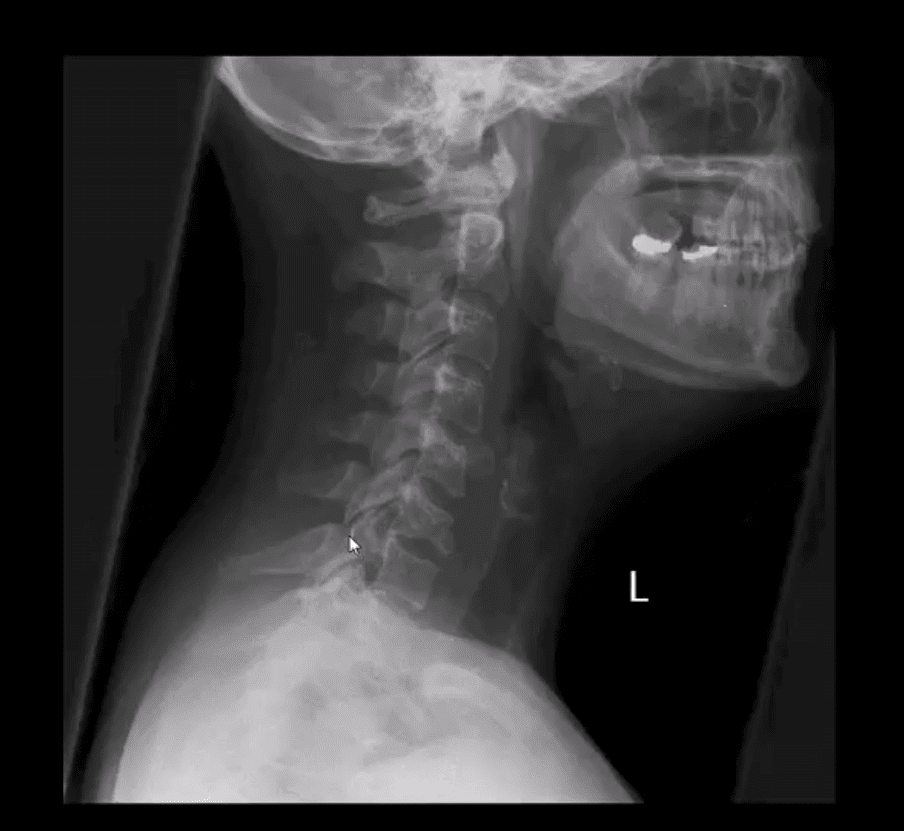
- CT scanning w/o contrasts with sagittal reconstruction. Note C7 Flexion teardrop Fx.
- CT may help with further delineation and preoperative planning
- May follow with MR imaging and evaluation of the neurological injury
- Fluid sensitive (T2) sagittal MRI slice of Flexion teardrop fracture at C4 and possibly C5
- Note high signal intensity lesion in the cord and surrounding ligaments indicating cord edema and ischemia
- Management: neurosurgical with spinal fusion
- Complications:
- Quadriplegia/paraplegia
- Respiratory complications
- Disability, changes in the quality of life
- Decreased life expectancy

- Bilateral facet dislocation (unstable)
- Mechanism: Flexion-distraction injury
- Key radiography: anteriorly displaced body 50% or more
- Facets override and locked (can be perched left image)
- Major tearing of ligaments
- Chances of severe cord compression and paralysis
- Patients with ligaments laxity and degenerative changes are at higher risk
- Initial x-radiography is the first step
CT scanning w/o Contrast is Crucial:
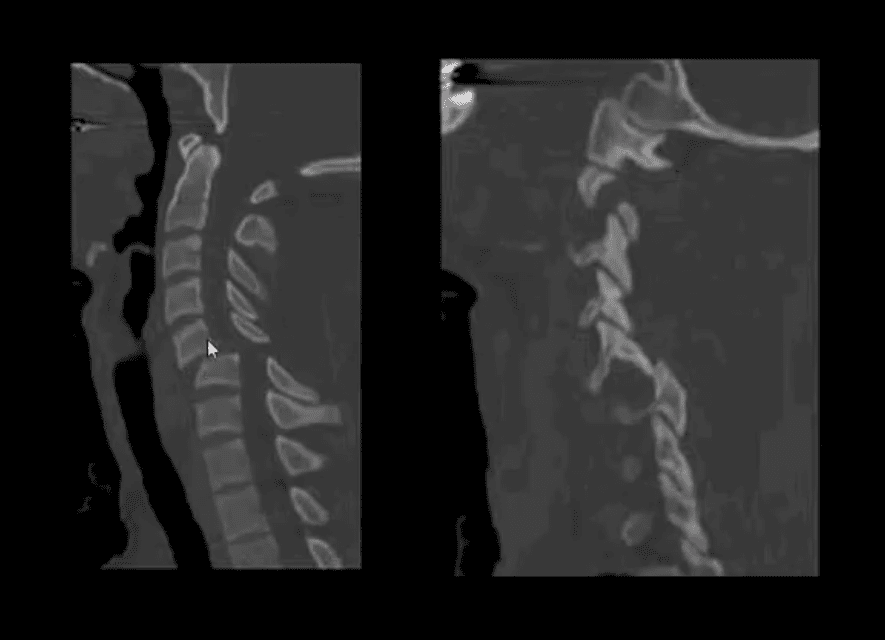
- Further delineation of this injury
- Facet fractures, pedicle fracture
- Management planning
Sagittal fluid sensitive MRI of bilateral C5 facet dislocation, sizeable ischemic cord injury, and posterior soft tissue injuries

- Management:
- X-radiography, then CT scanning then immediate closed reduction (esp. if the patient is conscious)
- Followed in some more complicated cases by MRI and then surgical care
- If the patient is awake and neurologically stable, CT and closed reduction are adequate
- Complicated cases and failed closed reduction may require surgical stabilization
- Complications: spinal cord injury and paralysis
- Delayed ligamentous laxity and instability
-
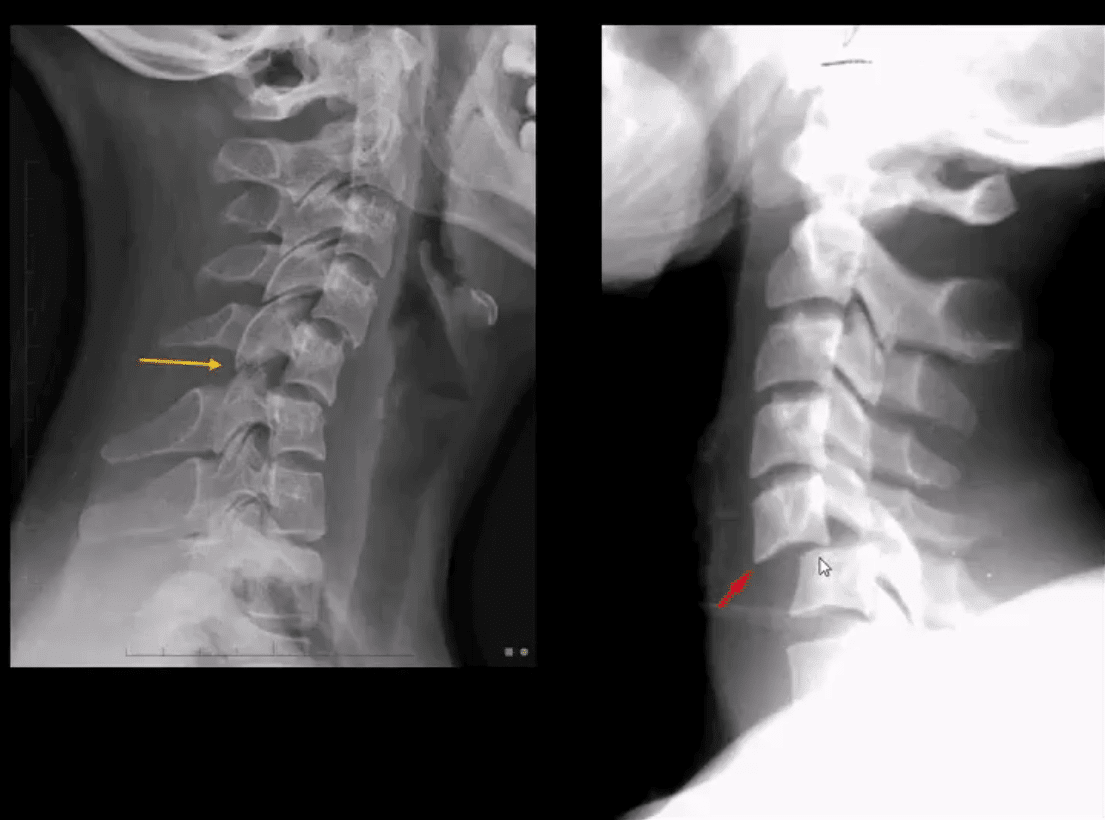
- Unilateral facet dislocation (flexion-rotation injury) less severe than bilateral dislocation
- Most commonly missed unstable cervical injury on x-radiography
- Key rad features: body anteriorly translated 25% facets appear misaligned and blurred, SPs rotated on frontal views
- Clinically may be presented as one-sided radiculopathy esp. C6 or C7
- CT scanning is required to evaluate further facet/pedicle fractures
- Pre-reduction evaluation and care planning
- Management: closed reduction esp. in a conscious patient
- Complications: acute disc herniation/retropulsion, ligamentous laxity, neurological injury
Spinal Trauma Imaging Approach
Resources:
- emedicine.medscape.com/article/824380-overview
- emedicine.medscape.com/article/248236-overview#a9
- emedicine.medscape.com/article/397896-overview#a3
- www.aafp.org/afp/1999/p331.html
Professional Scope of Practice *
The information herein on "Spinal Trauma Imaging Approach to Diagnosis Part I" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Our information scope is limited to Chiropractic, musculoskeletal, physical medicines, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somatovisceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and/or functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez, DC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, RN*, CCST, IFMCP*, CIFM*, ATN*
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807, New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Florida
Florida License RN License # RN9617241 (Control No. 3558029)
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Dr. Alex Jimenez DC, MSACP, RN* CIFM*, IFMCP*, ATN*, CCST
My Digital Business Card





